Download
1 / 1
10 likes | 189 Vues
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) PATIENT DISCHARGE INSTRUCTION CHECKLIST: CAN WE DO BETTER? Maryann Rabusic-Wiedener, Shauna Johns, Tina Ainsworth, Debra Lundberg, Maureen Stewart, Barb Stolee, Dr. James McMeekin, Dr. Mouhieddin Traboulsi for the Calgary Health Region. BACKGROUND

E N D
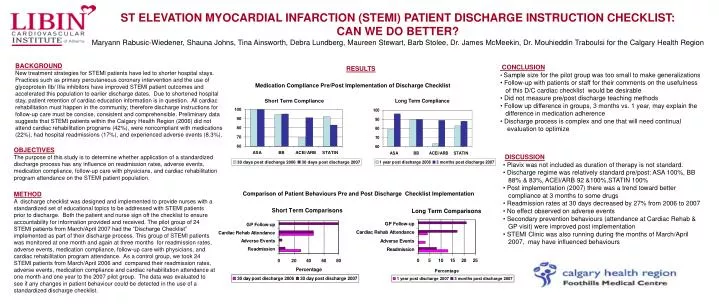
ST ELEVATION MYOCARDIAL INFARCTION (STEMI) PATIENT DISCHARGE INSTRUCTION CHECKLIST: CAN WE DO BETTER? Maryann Rabusic-Wiedener, Shauna Johns, Tina Ainsworth, Debra Lundberg, Maureen Stewart, Barb Stolee, Dr. James McMeekin, Dr. Mouhieddin Traboulsi for the Calgary Health Region BACKGROUND New treatment strategies for STEMI patients have led to shorter hospital stays. Practices such as primary percutaneous coronary intervention and the use of glycoprotein IIb/ IIIa inhibitors have improved STEMI patient outcomes and accelerated this population to earlier discharge dates. Due to shortened hospital stay, patient retention of cardiac education information is in question. All cardiac rehabilitation must happen in the community; therefore discharge instructions for follow-up care must be concise, consistent and comprehensible. Preliminary data suggests that STEMI patients within the Calgary Health Region (2006) did not attend cardiac rehabilitation programs (42%), were noncompliant with medications (22%), had hospital readmissions (17%), and experienced adverse events (8.3%). • CONCLUSION • Sample size for the pilot group was too small to make generalizations • Follow-up with patients or staff for their comments on the usefulness • of this D/C cardiac checklist would be desirable • Did not measure pre/post discharge teaching methods • Follow up difference in groups, 3 months vs. 1 year, may explain the • difference in medication adherence • Discharge process is complex and one that will need continual • evaluation to optimize RESULTS Medication Compliance Pre/Post Implementation of Discharge Checklist OBJECTIVES The purpose of this study is to determine whether application of a standardized discharge process has any influence on readmission rates, adverse events, medication compliance, follow-up care with physicians, and cardiac rehabilitation program attendance on the STEMI patient population. • DISCUSSION • Plavix was not included as duration of therapy is not standard. • Discharge regime was relatively standard pre/post: ASA 100%, BB • 88% & 83%, ACEI/ARB 92 &100%,STATIN 100% • Post implementation (2007) there was a trend toward better • compliance at 3 months to some drugs • Readmission rates at 30 days decreased by 27% from 2006 to 2007 • No effect observed on adverse events • Secondary prevention behaviours (attendance at Cardiac Rehab & • GP visit) were improved post implementation • STEMI Clinic was also running during the months of March/April • 2007, may have influenced behaviours METHOD A discharge checklist was designed and implemented to provide nurses with a standardized set of educational topics to be addressed with STEMI patients prior to discharge. Both the patient and nurse sign off the checklist to ensure accountability for information provided and received. The pilot group of 24 STEMI patients from March/April 2007 had the “Discharge Checklist” implemented as part of their discharge process. This group of STEMI patients was monitored at one month and again at three months for readmission rates, adverse events, medication compliance, follow-up care with physicians, and cardiac rehabilitation program attendance. As a control group, we took 24 STEMI patients from March/April 2006 and compared their readmission rates, adverse events, medication compliance and cardiac rehabilitation attendance at one month and one year to the 2007 pilot group. The data was evaluated to see if any changes in patient behaviour could be detected in the use of a standardized discharge checklist. Comparison of Patient Behaviours Pre and Post Discharge Checklist Implementation