Download
1 / 59
590 likes | 617 Vues
New Data on Treatment of ANCA-associated Vasculitis. C Salvarani, N Pipitone, G Germanò, MG Catanoso, F Muratore Unità di Reumatologia, Università di MO e RE e Azienda Ospedaliera-IRCCS di RE. Therapy of AAV: RCTs.

E N D
New Data on Treatment of ANCA-associated Vasculitis C Salvarani, N Pipitone, G Germanò, MG Catanoso, F Muratore Unità di Reumatologia, Università di MO e RE e Azienda Ospedaliera-IRCCS di RE
Therapy of AAV: RCTs Conventionalimmunosuppressiveagents and biological agents treatment - GPA and MPA - EGPA
Conventional Immunosuppressive Agents in GPA and MPA
Wegener’s granulomatosis: Early Outcomes Natural History: - Mean survival time: 5 months - Mortality: 82% in 1 year Glucocorticoid-treated generalized WG - Mean survival time: 12.5 months Fauci S and Wolff SM, Medicine 1973
The Fauci-Wolff Protocol: NIH Longitudinal Series (began 1968) Cyclophosphamide (CYC) 2 mg/Kg/day Glucocorticoids: - Pulse methylprednisolone (1g/day X 3) - Prednisone 1 mg/Kg/day - Tapered to qod after 3 months Typical duration of therapy: - Glucocorticoids: 12 months - CYC: Remission + 12 months Hoffman GS et al, Ann Intern Med 1992
CYC Therapy for AAV: The Good/The Bad 91% marked improvement 75% complete remission 42% permanent morbidity - 46% serious infections - 43% hemorrhagic cystitis - 33-fold risk of bladder CA - 11-fold risk of lymphoma - 57% infertility Steroid-induced damage: Cushingoid features, weight gain, hypertension, cataracts, fractures Hoffman et al, Ann Intern Med 1992
Conventional therapy for AAV How can we minimize exposure to CYC? How can we avoid CYC?
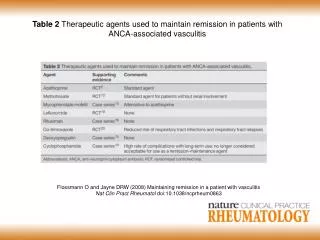
Lessons Learned from RCTs A short course of CYC for remission induction, followed by a longer course of MTX or AZA is an effective treatment strategy for AAV MMF was less effective than AZA for maintaining remission after induction of remission with CYC and PDN MMF is non-inferior to CYC for remission induction, but resulted in higher relapse rate, particularly in PR3-ANCA+ pts Jayne D et al, N Engl J Med 2003 (CYCAZAREM) Pagnoux C et al, N Engl J Med 2008 (WEGENT) Hiemstra TF et al, JAMA 2010 (IMPROVE) Jones et al, Ann Rheum Dis 2019 (MYCYC)
Lessons Learned from RCTs The pulse CYC (15 mg/kg pulse q2wkX3, then q3wk) induces remission as well as the daily oral regimen at a reduced cumulative CYC dose and causes fewer cases of leukopenia MTX (20-25 mg/wk) is appropriate for induction of remission for pts with mild form of vasculitis (non-renal), but may be associated with a higher risk of relapse de Groot K et al, Ann Intern Med 2009 (CYCLOPS) de Groot K et al, Arthritis Rheum 2005 (NORAM) Faurschou et al, Arthritis Rheum 2012 (NORAM extension)
Lessons Learned from RCTs Prolonged remission maintenace therapy with AZA/PDN , beyond 24 months after diagnosis, reduces relapse risk out to 48 months and improve renal survival Karras et al, Ann Rheum Dis 2017
Therapy of AAV: RCTs Biologic agents - TNF-blockers (etanercept) - Rituximab
Wegener’sGranulomatosisEtanercept Trial (WGET) • Etanercept in addition to standard therapy is not effective for the maintenance of remission in pts with WG • No difference in time to remission • No difference in frequency of remission • No difference in duration of remission • No difference in severity or frequency of flares • Increased risk of cancer in patients treated with etanercept (6 vs 0, P = 0.01) • WGET Research Group, N Engl J Med 2005
Pathogenic immune mechanisms in AAV Chen M & Kallenberg CGM, Nat Rev Rheumatol 2010
RTX in AAV • Remission - induction - maintenance
RTX versus CYC in ANCA-Associated Renal Vasculitis (RITUXVAS) Jone RB et al, N Engl J Med 2010 Randomized (3:1), controlled, open-label 44 patients All ANCA-positive, all new diagnosis All had severe renal disease Comparing: RTX plus 2 infusions of CYC (n=33) Intravenous CYC for 6 months, followed by oral AZA (n=11) Everybody remained on ~ 10 mg/day of prednisone Primary endpoints: sustained remission at 12 months and severe adverse events
Main RITUXVAS Results No difference between treatment arms of: Mortality: 18% in each arm Sustained remission at 12 months: - RTX 76% vs CYC 82% Time to remission: RTX 90 days vs CYC 94 days Relapse rate Time to relapse Improvement of renal function Adverse events rate Conclusion: over 12 months one course of RTX achieves the same results as 6 months of CYC followed by AZA Jone RB et al, N Engl J Med 2010
RTX versus CYC for ANCA-Associted Vasculitis (RAVE) Stone JH et al, N Engl J Med 2010 • Randomized (1:1), double blind • 197 patients (newly diagnosed or relapsing disease) • All ANCA-positive • Limited disease (not requiring CYC) and too severe disease (mechanical ventilation because of alveolar hemorrhage or serum creatinine > 4 mg/dL) were excluded • Comparing: • RTX plus daily placebo-CYC (n=99), then placebo-AZA for pts in remission between 3-6 months • Daily CYC (2 mg/Kg) plus placebo-RTX infusions (n= 98), then daily AZA (2 mg/Kg) for pts in remission between 3-6 months • Primary endpoint: remission without the use of prednisone at 6 month
Main RAVE Results No difference between treatment arms of: • Remission without the use of prednisone at 6 months: - RTX 64% vs CYC 53% - RTX 67% vs CYC 42% (p=0.01) for relapsing disease • Improvement of renal function • Adverse events rate • Loss of proteinase 3-ANCA production occurred more frequently with RTX than with CYC Conclusion: RTX was not inferior to daily CYC for induction of remission and may be superior in relapsing disease Stone JH et al, N Engl J Med 2010
Efficacy of Remission-Induction Regimens for AAV Specks et al NEJM 2013 The 18-month results of the RAVE study: • Maintaining complete remission at 12 and 18 months: - RTX 48% and 39% vs CYC/AZA 39% and 33% - RTX met the prespecified criteria for noninferiority (P<0.001,with a noninferiority margin of 20%) • No significant difference in the duration of complete remission and frequency or severity of relapses • Among the 101 patients who had relapsing disease at baseline: - RTX was superior to CYC/AZA at 6 months (P = 0.01) and at 12 months (P = 0.009) but not at 18 months (P = 0.06), at which time most pts had reconstituted B cells • No significant between-group difference in adverse events • Conclusions: a single course of RTX was as effective as continuous conventional immunosuppressive therapy for the induction and maintenance of remissions over the course of 18 months
Rituximab Dosage RITUXIVAS and RAVE trials used rituximab at a dose of 375 mg per square meter per week for 4 consecutive weeks However, in a retrospective evaluation of 65 sequential patients receiving RTX for refractory AAV there was no difference in efficacy between 4 infusions of 375 mg/m2 each given 1 week apart or 2 infusions of 1 gm each given 2 weeks apart Jones RB et al, Arthritis Rheum 2009
Rituximab is Effective in the Treatment of Refractory Ophthalmic WG • Initial small series showed that granulomatous orbital involvement was unresponsive to RTX • A beneficial response to RTX was seen in 10 patients with refractory scleritis (n=3) , orbital granulomas causing optic nerve compromise (n=4), or a combination of both conditions (n=3) Taylor SRJ et al, Arthritis Rheum 2009
Rituximab in Diffuse Alveolar Hemorrhage secondary to AAV Cartin-Ceba et al, Arthritis Rheumatol 2015 • Patients: 73 consecutive patients with AAV-associated DAH were evaluated at Mayo Clinic over a 16 year period • Results: • Rituximab treatment was independently associated with increased odds of achieving complete remission (BVAS/WG of 0 and PDN suspension) at 6 months (OR 6.45, 95%CI 1.78-29, p=0.003) • PLEX was not associated with achieving complete remission at 6 months (OR 0.49, 95%CI 0,12-1.95, p=0.32)
RTX in AAV: Remission maintenance therapy • 10% of pts treated with CYC + GCs have a refractory disease • In the RCT of prolonged treatment 63% of pts who suspended AZA/PDN by 24 months flared • In the WEGENT trial the relapse rate was 36% in the AZA group and 33% in MTX group after a mean follow-up of 29 months after remission • Booth et al, Am J Kidney Dis 2003; De Groot K et al Arthritis Rheum 2005; • Jayne et al, N Engl J Med 2003; Pagnoux et al, N Engl J Med 2008; Karras et al, Ann Rheum Dis 2017 • a single course of RTX induces sustained remission without the need for maintenance immunosuppression: • - in the French retrospective study 1-, 2- and 3-year relapse-free survival rates after the first infusion were 80%, 63% and 52% • Charles et al, Rheumatology 2014
Rituximab versus Azathioprine for Maintenance in ANCA-AssociatedVasculitis (MAINRITSAN) Guillevin et al, NEJM 2014 Methods: - Pts with newly diagnosed or relapsing disease in complete remission after CYC-steroid therapy were randomly assigned to receive a 500-mg RTX infusion on D1, D15, and at months 6, 12, 18 after study entry or daily AZA (2 mg/kg/d) until month 22 - Pneumocystis jiroveci pneumonia prophylaxis for CD4+ T-lymphocyte count < 250 mm3 Primary end point:rate of major relapse at month 28 Results: - 58 ptsreceived AZA and 57 RTX - atmonth 28, major relapse occurred in 3 pts (5%) in the RTX arm and in 17 pts (29%) in the AZA arm (p = 0.002) - 25 pts in each group had SAE Conclusion: - 500 mg of RTX every 6 months was superior to AZA
Long-term efficacy of remission-maintenanceregimens for ANCA-associated vasculitidesTerrier et al, Ann Rheum Dis 2018 For AZA and RTX groups, atmonth 60: • Major relapse-free survival: 49% vs 72% (p=0.003) • Minor and major relapse-free survival: 37% vs 58% (p = 0.01) • Overall survival rates: 93% vs 100% (p=0.045) • At multivariate analysis, PR3-ANCA positivity (HR 2.04) and AZA arm (HR 2.72) wereindipendentlyassociated with higher risk of relapse • 16 (28%) AZA group and 15 (26%) RTX group had severe infections: 3 PJP (1 AZA, 2 RTX), 2 Asp e 2 myc. inf.
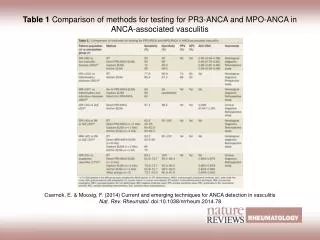
Clinical outcomes of treatment of ANCA-associated vasculitis based on ANCA type Unizony et al, Ann Rheum Dis 2015 • Methods: treatment responseswereassessedamongptsenrolled in the RAVE trial according to both AAV diagnosis (GPA or MPA) and ANCA type (PR3-AAV/MPO-AAV). Complete remission (CR): BVAS/WG of 0 and succesfulcompletion of the prednisone taper Results: • PR3-AAV ptstreated with RTX had CR at 6 months more frequentlythandidthoserandomized to CYC/AZA (65% vs 48%, p=0.04) with an OR of 2.11 (95%CI: 1.04-4,30) • PR3-AAV pts with relapsingdiseasehad CR more often with RTX at 6 months (OR 3.57), 12 months (OR 4.32), and 18 months (OR 3.06) • No associationbetween treatment and CR wasobserved in the MPO-AAV patients or in groups dividedaccording to AAV diagnosis
RTX for remission induction and maintenance in refractory GPA (Wegener’s) Cartin-Ceba et al, Arthritis Rheum 2012 • Methods: 10-year single-center observational study of all pts with chronic relapsing GPA treated with at least 2 courses of RTX • Results: • - 53 pts received at least 2 courses (median 4 courses) of RTX to treat relapses or to maintain remission • all had depletion of B cells (median time to return: 8.5 mo) • Relapses occurred after reconstitution of B cells and were accompanied or preceded by an increase in ANCA levels • 30 infections occurred during B cell depletion period (no SAEs) • Conclusion: Preemptive re-treatment decisions can be individualized based on serial B lymphocytes and PR3 ANCA monitoring
Comparison of individually tailored versus fixed-schedule RTX regimen to maintain ANCA-associated vasculitis remission: results of a multicentre, randomised controlled, phase III trial (MAINRITSAN2) Charles et al, Ann Rheum Dis 2018 • 162 pts with newly diagnosed or relapsing GPA or MPA in complete remission after induction therapy (CYC 100, RTX 61, MTX 1) • Tailored arm: RTX 500 mg at randomisation, with reinfusion only when CD19+B cells or ANCA reappeared or ANCA titre rose (twice) based on trimestrial testing until month 18 • Controls: fixed 500 mg RTX infusion on days 0 and 14 postrandomisation, then 6, 12 and 18 months after the first infusion • Primary end point: number of relapses at month 28 • At month 28, 21 pts had 22 relapses: 14/81 (17.3%) in 13 pts of tailored arm vs 8/81 (9.9%) in 8 fixed-schedule-infusion pts (p = 0.22) • 26 (32.1%) tailored-infusion pts vs 31 (38.3%) controls had at least one severe AE (p = 0.51) Relapse-free survival: 83.8% vs 86.4% (p=0.58)
Take-Home Message • Available data do no support the useofanti-TNFtherapy in AVV • Resultsfrom 2 RCTscomparing RTX to CYC complementeachother: - RTX iseffectiveas CYC for newlydiagnosedpts with severe AAV - RTX seem to be superior for pts with severe flares • RTX ispreferable: • - to preservefertility (youngpatients) • - in PR3-AAV pts with relapsingdisease
Take-Home Message • RTX iseffective in the treatment of refractory AAV, includingophthalmic GPA • RTX is more effectivethan AZA for maintainingremission in AAV, whilesafetyiscomparable • AAV relapse ratesdidnotdifferbetweenindividuallytailored and fixed schedule RTX regimens
Open Questions • in ptswithchronicrelapsingcourse re-treatment with RTX maysparethemadditionalmorbidity and damage: • - further RTX at the timeofrelapse • - re-treatment timing individualized on B cellcounts and/or ANCA levels • - routine fixed-interval re-treatment regimen • the benefit/riskratioofanimmunosuppressant (MTX or AZA)/RTX hasnotbeenevaluated • are low IgGlevels at baseline (21%) and duringfollowupassociatedwithincreasedinfections? • isPneumocystisjiroveci pneumonia (PCP) prophylaxiswithtrimetrophrim/sulfamethoxazolerecommended?
Should Pneumocystis jiroveci prophilaxis be recommended with RTX treatment in AAV? • the incidence of PJ pneumonia (PCP) is increased in pts with AAV compared with other CTDs • treatment with MTX, high-dose prednisolone, and CYC in association with lymphopenia increases the risk for PCP in GPA pts • prophylaxis with TMP-SMX is effective and EULAR recommends its use during CYC therapy in AAV • multiple reports of PCP developing in pts treated with RTX for hematological malignancies and few reports in patients treated with RTX for AAV • Mayo Clinic retrospective study 1998-2011: 30 pts developed PCP after RTX treatment (90% had hematological malignancies and 10% were only treated with RTX) • it is still unclear if PJ screening from induced sputum before RTX may help to identify pts in need of eradication and long-term prophylaxis • some experts in AAV recommends PCP chemoprophylaxis in pts treated with RTX continuously or for at least the duration of B cells depletion Besada and Nossent , Clin Rheumatol 2013; Hugle et al, Arthritis care & Res 2010; Clain et al, Ther Adv Musculoskel Dis 2014; Ognibene at al, Am J Respir Crit Care Med 1995; Martin-Garrido et al, Chest 2013; Ward et al, Arthritis Rheum 1999
Future Perspectives • Remissioninduction with 1 course of RTX, 3 months of low-dose CYC (6 pulses 500 mg every 2 ws) and a short course of oral GC (for between 1 and 2 weeks) waseffectiveas the standard of care and wasassociated with less GC-relatedAEs Pepper et al, Rheumatology 2019 • In a RCT avacopan (CCX168), an orallyadministeredselective C5a receptor inhibitor, waseffective in replacing high-dose GCswithoutcompromising the efficacy of CYC or RTX Jayne et al, J AmSocNephrol 2017
Future Perspectives • In an open-labeltrial of pts with non-severe relapsing GPA, abatacept, a recombinant fusion protein that modulates CD28-mediated T-cell costimulation,wasassociated with a high frequency of remission and PDN discontinuation Langford et al, Ann RheumDis 2014 • Belimumab, a IgG1λmonoclonal Ab againstBlyS, plus AZA and GCs for the maintenance of remission in AAV didnot reduce risk of relapse Jayne et al, Arthritis & Rheumatology 2019
Eosinophilic Granulomatosis with Polyangiitis (Churg-Strauss)
Five Factor Score: Therapeuric Stratification According to Prognosis FFS: Guillevin et al, Medicine 1996 • Proteinuria > 1 g/d • GI bleeding, perforation, infarction, and/or pancreatitis • Renalinsufficiency (Cr > 1.58 mg/dL) • CNS involvement • Cardiomyopathy FFS revisited: Guillevin et al, Medicine 2011 • Age > 65 years • Cardiacinsufficiency • Renalinsufficiency (> 150 umol/L = 1.7 mg/dL) • Gastrointestinalinvolvement • Absence of ear, nose, throat (ENT) involvement Everymanifestationwasscored +1 point whenpresent
Treatment of Churg-Strauss Syndrome Without Poor-Prognosis Factors Ribi et al, Arthritis Rheum 2008 Prospective, multicenter, randomized trial: • to assess the efficacy of GCs (PDN 1 mg/Kg/day) alone as first-line treatment in EGPA without poor prognosis factors (FFS: 0) • to compare oral AZA versus iv pulse CYC asadjuvanttherapy for treatment failure or relapse • At treatment failure or relapse pts were randomized to receive 6 months of oral AZA or 6 pulses of CYC
Treatment of Churg-Strauss Syndrome Without Poor-Prognosis Factors Ribi et al, Arthritis Rheum 2008 • 93% achieved remission and 35% flared • among the 19 pts randomized, 5/10 receiving AZA and 7/9 receiving pulse CYC achieved remission (p = NS) • at the end of follow-up, 79% of the pts whose disease was in remission required low-dose GCs, mainly to control respiratory disease Meanfollowup: 56.2 months
Adding Azathioprine to Remission-Induction Glucocorticoids for Eosinophilic Granulomatosis With Polyangiitis (Churg-Strauss), Microscopic Polyangiitis, or Polyarteritis Nodosa Without Poor Prognosis Factors Puéchal et al, Arthritis & Rheumatology 2017 • 95 pts with newly diagnosed EGPA:51, MPA:25 , PAN:19 • All patients received GCs, gradually tapered over 12 months, and were randomized to receive AZA or placebo for 12 months • Primary end point: pts with refractory or relapsing disease at month 24 • Primary outcome at 24 months: • patients with relapse or refractory disease: AZA 47.8% (n = 22) versus PBO 49% (n = 24) (p=0.86) • Secondary outcomes: • no differences in BVAS, HAQ and VDI and cumulative PDN dose • post-hoc analysis on EGPA pts same results • in EGPA comparable % of pts with asthma/rhinosinusitis exacerbations (AZA: 24%, PBO:19.2%) • Safety: • No differences between groups
No GC-sparingeffect of AZA Puéchal et al, Arthritis & Rheumatology 2017
Churg-Strauss Syndrome With Poor-Prognosis Factors: A Prospective Multicenter Trial Comparing Glucocorticoids and Six or TwelveCyclophosphamide Pulses in Forty-Eight PatientsCohen et al, Arthritis Rheum 2007 • Prospective multicenter trial including 48 newly diagnosed EGPA pts with at least 1 poor prognosis factor (FFS > 1) • Pts treated with PDN (1 mg/Kg/day) and either 12 or 6 iv CYC pulses (interim analysis at 4 years, final at 8 years)
Churg-Strauss Syndrome With Poor-Prognosis Factors: A Prospective Multicenter Trial Comparing Glucocorticoids and Six or TwelveCyclophosphamide Pulses in Forty-Eight PatientsCohen et al, Arthritis Rheum 2007 • Need for a maintenance therapy to prevent relapses in EGPA pts with at least 1 poor-prognosis factor • The optimal duration of therapy remains to be determined Mean follow-up: 42.5 months
Treatment of EGPA before Biologic Era • Therapeuticregimenbased on prognosisstratificationusingFiveFactor Score
Long-term outcome with this therapeutic regimen Outcomes: • 92% entered in remission • 29% achieved long-termremission • Death: 10% at 7 years Sequelaeat last visit in 86% of pts: • Chronicasthma: 83% • Peripheralneuropathy: 45% • Chronicrhinitis/sinusitis: 35%/19% • Osteoporosis: 30% 82% of ptswerestillreceivingoralGCs (mean dose: 10 mg/daily) at the last visit (mean follow-up duration: 81.3 months) Samson et al, J Autoimmun 2013; Comarmond et al, ArthrtisRheum 2013
Mepolizumab or Placebo for EosinophilicGranulomatosis with Polyangiitis Wechsler et al, NEJM 2017 • Multicenter, double blind, parallel-group, phase 3 trial • Randomization of EGPA pts with relapsing or refractory disease to receiveve 300 mg of mepolizumb or placebo plus standard of care for 52 weeks
Mepolizumab or Placebo for EosinophilicGranulomatosis with Polyangiitis Wechsler et al, NEJM 2017
Mepolizumab or Placebo for EosinophilicGranulomatosis with Polyangiitis Wechsler et al, NEJM 2017 During weeks 48 through 52, 44% receivingmepolizumabtaperedGCs to < 4.0 mg/day compared with 7% receiving placebo and 18% receivingmepolizumabdiscontinuedGCscompared with 3% receiving placebo