Basic Science – “Large Bowel”
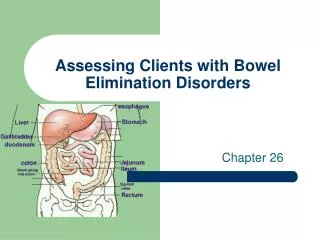
Basic Science – “Large Bowel”. Anatomy. Right colon Transverse colon Left colon Descending Sigmoid Rectum What defines the transition between the sigmoid colon and rectum?. Colon - Anatomy. What are the layers of the bowel wall? What comprises the tenia?.

Basic Science – “Large Bowel”
E N D
Presentation Transcript
Anatomy • Right colon • Transverse colon • Left colon • Descending • Sigmoid • Rectum • What defines the transition between the sigmoid colon and rectum?
Colon - Anatomy • What are the layers of the bowel wall? • What comprises the tenia?
Colon - Physiology • What is the primary role of the colon? • Fluid absorption • 900ml of water • Bile acids • Sodium (active transport)
Colonic transit • R colon: segmental propulsive & retropulsive contractions for “mixing” • L colon: mostly propulsive contractions • “Mass movements”: large peristaltic contractions (1-3/day) that move contents about 1/3 the length of the colon
Defecation • Distention of the rectum triggers the rectoanal inhibitory reflex (RAIR): • External anal sphincter voluntarily relaxed • Rectum / Distal colon contract • Pelvic floor relaxes (straightening of rectosigmoid angle)
Diverticular Disease True or false diverticula?
Acute Diverticulitis (simple) • Symptoms • LLQ abdominal pain/fever/leukocytosis • Radiologic evaluation • CT scan • Treatment • Bowel rest & IV ABX • Duration of both?
Acute Diverticulitis (simple) • Management after resolutions of symptoms: • BE or Colonoscopy 6-8 wks later • Discussion re: surgical intervention What are the proximal and distal margins in an elective resection for diverticulosis?
Complicated Diverticulitis • Perforation • Abscess/Phlegmon/Peritonitis • Obstruction • Acute inflammation vs. fibrosis • Fistula • Colovesical/Colovaginal • Bleeding
Complicated Diverticulitis - Management • Perforation • With contained abscess • With peritonitis • Obstruction • Acute • Chronic • Fistula • Bleeding
Ulcerative Colitis • Inflammatory condition of the colon and rectum limited to the mucosa and submucosa • Etiology: unknown • Age of onset: Bimodal distribution
Ulcerative Colitis • Disease begins at the dentate line and move proximally without skip areas • 75% confined to proctosigmoiditis • Symptoms: • Numerous bloody bowel movements • “no blood, no UC” • Abdominal pain and cramps • Tenesmus, fecal urgency & incontinence
Ulcerative colitis – Medical Management • Tailored to disease severity • Mild –Moderate disease • Sulfasalazine and its derivatives (mesalamine based compounds) • Immunosuppressives (6-MP, Azathioprine) • Severe disease • Corticosteroids • Cyclosporine A
Ulcerative colitis – Indications for surgery • Elective Intractability Dysplasia, malignancy or malignancy prophylaxis Complications of medications (usually steroids) • Emergency Toxic colitis Hemorrhage Acute exacerbation unresponsive to medical Tx
Emergency Subtotal colectomy with end-ileostomy Elective Proctocolectomy + End ileostomy IPAA Koch pouch Ulcerative Colitis – Surgical options
Crohns Disease • Inflammatory condition of the GI tract of unknown etiology • Bimodal distribution • “mouth to anus” • Skip areas • Transmural • Non-caseating granulomas
Crohns Disease - symptoms • Crampy abdominal pain • Watery diarrhea • Fecal urgency and tenesmus
Crohns Colitis – Endoscopic features • Skip areas – often with rectal sparing • “cobblestone” appearance • Serpigenous ulcerations
Crohns disease -Treatment • Medical management is the mainstay of Crohns disease: • Mild / Moderate disease: 5-ASA compounds • Severe disease: Steroids • 6-Mp and Azathioprine for maintenance
Crohns disease - complications • Abscess • Fistula • Perforation • Toxic colitis • Obstruction • Colonic stricture = malignancy
Crohns Disease - Surgery • Goal: To palliate the symptoms • Location and extent of disease determine operative procedure in Crohns colitis: • Segmental resection vs. proctocolectomy
Large Bowel Obstruction • Etiology: Colon cancer (Left-sided) Volvulus (cecal & sigmoid) Diverticulosis
Large Bowel Obstruction - Presentation • Symptoms • Obstipation, abdominal pain and distention, +/- emesis • Physical Exam • Abdominal distention, tenderness,
Large Bowel Obstruction - Management • Resuscitation • X-Rays… • Plain films • Retrograde GGE • CT scan • …vs. Endoscopy
Large Bowel Obstruction - Management • Sigmoid Volvulus • Cecal volvulus • Malignancy (Left side) Hartmann procedure Resection/ on-table lavage/ primary anastomosis Subtotal + anastomosis ? Stent
Colon cancer – Inherited • Familial adenomatous polyposis • Autosomal Dominant (APC gene: 5q21) • Scattered polyps to “carpeted” • 100% lifetime risk of developing cancer without surgery • Extraintestinal manifestations (Gardner’s syndrome) • Desmoids/CHRPE/periampullary ca/epidermal cysts
Colon cancer – Inherited • FAP – Surgical treatment • Proctocolectomy with • End ileostomy • IPAA • Subtotal colectomy / IRA • +/- Sulindac
Colon cancer – Inherited • HNPCC (Lynch Syndrome) • Autosomal dominant • Germline mutation in DNA mismatch repair genes (hMLH1, hMSH2) • Scattered polyps with tendency toward proximal lesions • 80% lifetime risk of developing colon cancer • Amsterdam criteria • Extracolonic malignancies • Endometrial/Ovarian/GU Surgical management: Subtotal / IRA
Non-neoplastic Hyperplastic Juvenile Inflammatory Neoplastic potential Villous adenoma Tubular adenoma Tubulovillous adenoma Colon cancer - polyps Which has the highest malignant potential?
Colon cancer – Sporadic Adenoma to carcinoma:
Colon cancer - presentation • Bleeding • Anemia • Guaiac + • Obstruction • Screening
Colon cancer – pre-op evaluation • Family history! • CEA • Colonoscopy • Tissue for diagnosis • Evaluate remainder of colon • Abdominal/Pelvic CT scan • ? PET scan
Colon cancer – adjuvant therapy • Stage III • 5-FU / Leucovorin based • ? Stage II with adverse features • Poorly differentiated • LVI • Obstruction/Perforation
Colon cancer - surveillance No survival benefit with aggressive surveillance strategies!