Endothelial Progenitor Cells (EPCs)
Endothelial Progenitor Cells (EPCs). EPCs in CV diseases. CV risk factors Endothelial dysfunction Collaterals Restenosis CV disease. EPCs. Pathophysiology. Therapeutics. Atherosclerosis Heart disease Peripheral vascular disease. Courtesy of Arshed A. Quyyumi, MD.


Endothelial Progenitor Cells (EPCs)
E N D
Presentation Transcript
EPCs in CV diseases CV risk factors Endothelial dysfunction Collaterals Restenosis CV disease EPCs Pathophysiology Therapeutics Atherosclerosis Heart disease Peripheral vascular disease Courtesy of Arshed A. Quyyumi, MD.
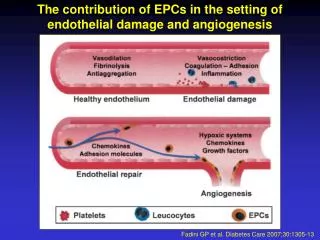
Circulating EPCs aid in cardiac repair • CD34+, CD133+, and VEGF2R+ • Circulate in blood stream • Contribute to repair of vascular or myocardial injury and collateral formation Asahara T et al. Science. 1997;275:964-7. Takahashi T et al. Nature Med. 1999;5:434-8.
EPC physiology • Originate in bone marrow • Circulate in blood stream • Number and function (proliferation, migration, homing) modulated by age, CV risk factors, and disease • Release stimulated by organ and vascular injury • Participate in vascular repair (collateralization) and re-endothelialization, partly by paracrine effects • Circulating numbers by exercise and drugs (statins and ACE inhibitors) • Independent predictors of endothelial dysfunction and long-term prognosis in patients with CAD Hill JM et al. N Engl J Med. 2003;348:593-600.
EPC number has prognostic importance N = 519 males with CAD, mean age 66 y 1.00 Group 3 (high EPC level) 0.98 0.96 Group 2 (medium EPC level) Event-free survival 0.94 Group 1 (low EPC level) 0.92 0.90 0 0 100 200 300 365 Days Werner N et al. N Engl J Med. 2005;353:999-1007.
Association between CV risk factors and EPC colony counts N = 45 males without CAD, > 21 years (mean age 50.3) 70 r = –47.0 P = 0.001 60 50 40 EPC colony-forming units 30 20 10 0 -5 0 5 10 15 20 Framingham risk score Hill JM et al. N Engl J Med. 2003;348:593-600.
Mobilization of EPCs after myocardial infarction N = 16 patients with AMI, 8 controls P < 0.001 P < 0.001 P < 0.001 P < 0.05 300 200 MNCCD34+ (/106WBCs) 100 0 Day 1 3 7 14 28 Time after onset Shintani S et al. Circulation. 2001;103:2776-9.
VEGF levels correlate with increase in EPCs 450 r = 0.35 P = 0.01 400 350 300 250 200 MNCCD34+(cells/106 WBCs) 150 100 50 0 0 50 100 150 200 250 300 350 400 450 Plasma VEGF (pg/mL) Shintani S et al. Circulation. 2001;103:2776-9.
EPC activity and coronary collaterals A P = 0.017 0.4 0.3 0.2 CD34/CD133 Dual PositiveCells (% of total lymphocytes) 0.1 0 Colln=13 Colln=10 • 30 patients with isolated left anterior descending disease • Divided into groups with (0.33) and without (0.09) adequate Collateral Flow Index (CFI) B R = 0.75P < 0.0001 0.8 0.6 CD34/CD133 Dual PositiveCells (% of total lymphocytes) 0.4 0.2 0 0 0.1 0.2 0.3 0.4 0.5 CFI Inadequate coronary collateral development associated with ¯ numbers of circulating EPCs and impaired chemotactic and pro-angiogenic activity Lambiase PD et al. Circulation. 2004;109:2986-92.
Decrease in EPCs associated with CV disease Endothelial Progenitor Cells Vasculoprotective agents CV risk factors Atherosclerosis Disease Regression? Disease Progression Improvement of endothelial function Enhanced re-endothelialization Reduced plaque size Improved angiogenesis Myocardial infarction Ischemic stroke Erectile dysfunction Renal insufficiency Peripheral artery disease Werner N, Nickenig G. Arterioscler Thromb Vasc Biol. 2006;26:257-66.