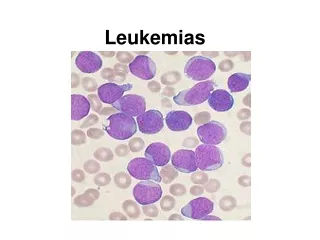
Leukemias
Leukemias. Jan Żeromski Pathology 2010/2011. Definition and two main lineages. Malignant proliferation of white cells of the hematopoietic system with infestation of blood and usually bone marrow. Lymphoid and myeloid leukemias. Cell origin and pathogenesis.

Leukemias
E N D
Presentation Transcript
Leukemias Jan Żeromski Pathology 2010/2011
Definition and twomainlineages • Malignant proliferation of white cells of the hematopoietic system with infestation of blood and usually bone marrow. • Lymphoid and myeloid leukemias
Cellorigin and pathogenesis • Hematopoieticstemcellsdifferentiating to progenitorones, eithermyeloidorlymphoidlineage • Chromosomalabnormalities, most commonlytranslocations, • Inheritedgeneticdefects (Down syndrome, Bloomsyndrome, ataxiatelangiectasia • Someviruses: Epstein-Barr (EBV), herpesvirus -8, HTVL-1 etc. • Environmentalfactors: chronicinfection, Helicobacterpylori, radiationtherapy, chemotherapy
Classification of lymphoidleukemias • Precursorleukemias - acutelymphoblastic l. - pro B - pre B (common) • Peripheralones - chroniclymphocytic l. - prolymphocytic l. - hairycell l. - plasmacellmyeloma • Precursor leukemias - acute lymphoblastic l. • Peripheral ones (T and NK) - chronic lymphocytic l. - large granular lymphocytic l. - Sezary syndrome - NK-cell leukemia B-cell origin T-cell origin
Significance of cellimmunophenotype • Definition:the set of differentiationantigensexpressed on a givencelltype • Lymphoid and myeloidcellsubsetsinvariousstages of maturationhavedistinctimmunophenotype • Differentiationantigensareclassifiedaccordingto clusterdeterminants (CD) system • CD classificationcoversmorethan 300 antigenicepitopessearched by monoclonalantibodies • Each leukemia typehascharacteristic set of CD markers, whatconstitutesnowadayscurrentclassificationhematopoieticmalignancies and thebasis of diagnosis
B cell lineage antigens differentiation
Clonality – generearrangement • Clonality – crucialdifferencebetweenneoplastic and normallymphocytes • Uniquefeature of lymphocytes – antigen receptor • Antigen receptor generearrangementdetermines antigenspecificity of lymphocytes • Rearrangementprecedesneoplastictransformation • Thusdaughtercellsfrommalignantcellprogenitorexpressthe same antigen receptor (either T or B) – form identicalcell clone
Acute Lymphoblastic Leukemia • Most cases are Tdt positive • Most express CD10 (common ALL antigen) • Most are “pre-B cell” phenotype • 15-20% T-cell lineage • 5% B-cell phenotype
General division of myeloidneoplams • Acute myelogenous leukemias (8 types) • Myelodysplastic syndromes (MDS) • Chronic myeloprolifeative disorders: - chronic myelogenous leukemia - polycythemia vera - essential thrombocytosis - primary meylofibrosis
FAB classification of acutemyelogenousleukemias • M0 AML – non-differentiated, incidence 2-3% • M1 AML – almostwithoutdifferentiation, 20% • M2 AML – myeloidmaturation of granuloc.30-40% • M3 AML – hypergranularpromyelocytes, 5-10% • M4 AML – cells of bothmyelocytic (min.20%) and monocyticorigin (<30%), 15-20% • M5 AML – Monoblasts (M5a) and monocytes (M5b), 10% • M6 AML – dysplasticerythroidprecursors and myeloblasts, 5% • M7 megakaryocytic leukemia – blasts of megakaryoc.lineagepredominate, 1% Number of blastsinall: < 20%
Myeloid cell lineage antigens differentiation
Significance of geneticabnormalities • Chromosomaltranslocationisfairlycommon and may be distinct for givensubtypesuch as t(15;17) in M3 AML • Someleukemias do no fit to currentclassifications and aredescribed on thebasis of severalcytogeneticdefectssuch as genefusion, deletion, insertion etc. • In lymphoidtumorsantigen receptor generearrangementisearlierthanneoplastictransformation. Thus, tumorousgene products (immunoglobulinsorT-cellreceptors) areidenticalincontrast to normallymphocytesexpressingplethora of variousantigenreceptors. Itturned out to be of diagnosticvalue.
Clinicalfeatures of leukemias • General: symptomsaremoreevidentinacutethaninchronicforms , but do not differ much inlymphoidvs. myeloidleukemias, • In chronictypestheonsetisusuallyinsidious: mild anemia, weakness, easyfatigue, weightloss, anorexia • Enlargement of spleen iscommoninbothtypesoften associated withleftupperquadrantpain, • Acuteleukemias manifest by abruptstormyonset: fever, infection, bleeding, bonepain, hepatosplenomegaly, cnsmanifestationssuch a vomiting, headache, nervepalsies.
Chronic Leukemia • Often discovered because of an abnormal lab or an abnormal physical examination • Severe cytopenias characteristic of acute leukemia are seldom present at time of diagnosis
Prognosisinleukemias • FairlygoodinprecursorB-cellleukemiasinchildhood • In chronicB-cellleukemias life expectancymay be comparable to normal one, providedthatthereis no cnsinvolvement • Acutemyeloidleukemiashaveusuallyunfavourableprognosis (15-30% remainfree of disease for 5 years), • In chronicmyelogenous leukemia supplementation of blood and properchemotherapyallowfro 4-5 yearssurvival, but theendisalmostalwaysfatal.
HairyCell Leukemia (HCL) • Clinical – pancytopenia, normal lymph nodes and splenomegaly • Incidence –mostly middle age males (2% of lymphomas) • Origin – mature B cells but with peculiar projections best seen in phase-contrast microscope. They are pan B, CD5-, CD25+, CD11c+, CD103+ • Infiltration of spleen, bone marrow and liver • Accompanying infections common often with atypical mycobacteria
FAB classification of acutemyelogenousleukemias • M0 AML – non-differentiated, incidence 2-3% • M1 AML – almostwithoutdifferentiation, 20% • M2 AML – myeloidmaturation of granuloc.30-40% • M3 AML – hypergranularpromyelocytes, 5-10% • M4 AML – cells of bothmyelocytic (min.20%) and monocyticorigin (<30%), 15-20% • M5 AML – Monoblasts (M5a) and monocytes (M5b), 10% • M6 AML – dysplasticerythroidprecursors and myeloblasts, 5% • M7 megakaryocytic leukemia – blasts of megakaryoc.lineagepredominate, 1% Number of blastsinall: < 20%
AcuteMyelogenous Leukemia (AML) • Incidence:middleage, olderadults and children • Bonemarrow: normalcellsarereplaced but undifferentiatedblastswithsomemyeloidfeatures. Theyhaveblockedmaturation, increasedsurvival and thereplicationratelowerthannormalmyeloidprogenitors, • Genetic:severalchromosomalrearrangementsdisruptinggenesencodingtranscriptionfactorsneeded for normalmyeloidmaturation, • Lab findings: anemia, neutropenia, thrombocytopenia
AcuteMyelogenous Leukemia (AML) - 2 • Flowcytometry:due to poorcellgranularityblastshaveverylowsitescatter. Theyusually show myeloid-specificsurfacemarkers (CD13, CD33) and markers of progenitorcells (CD34, CD117), but variousdeparturesfromtheabovearecommon, • Clinical:fatigue, spontaneousbleedings, infections, oftencaused by opportunisticpathogenssuch as fungiorPseudomonas. Organomegaly of liver, spleen, infiltration of skin, gingiva by normalmonocytesisoftenseen.
Platelet Coagulation Petechiae, Purpura Hematoma, Joint bl.
Chronicmyelogenous leukemia (CML) • Disease of adults(25 – 60 yrs), morecommoninwomen, • Bonemarrow– highlycellular, mainlymaturinggranulocyteprecursors, increasednumbers of megakaryocytes • Molecular– translocation of BCR gene (chromosome 9) to ABL gene (on chromosome 22) TheresultantBCR-ABLfusiongeneencodes protein withtyrosinekinaseactivity. So-called Philadelphia chromosomeseeninkaryotypingstudiesisthereflection of (9;22) translocation • Clinical – slow progressionup to 5 years, afterwardssome 50% of patients enter „acceleratedphase” withappearance of blasts, resemblingacute leukemia.
BCR-ABL translocation Chronic Myelogenous Leukemia
BCR – ABL GENES DISRUPTED IN THE t(9;22) CHROMOSOMAL ABNORMALITY
PolycythemiaVera • Cellorigin: multipotentmyeloidstemcell • Bonemarrow: increasedproduction of erythroid, granulocytic and megakaryocyticmaturingcelltypes • Blood: erythrocytosis, granulocytosis, thrombocytosis, increasedhematocrit and red cell mass • Clinical:insidiousonsetinlatemiddleage (above 60 yrs). Patientssufferfromheadache, dizziness, hypertension, gastrointestinalabnormalities, goutdue to high cellturnover. Thrombosis episodesarecommon. • Finalfate: either „spentphase” leading to marrowmyelofibrosiswithextramedullaryhematopoesisor terminal AML
MyelodysplasticSyndromes (MDS) • Definition:clonalcelldisordersmarked by maturationdefects, ineffectivehematopoiesis and increasedrisk of AML (10-40%) • Twodistincttypes: idiopatic (primary) MDS inolderpeoplewithinsidiouscourse. Oftendiscoveredincidentally on routinetesting. therapy-related MDS, due to previouschemo-orradiationtherapy, usually 2 to 8 yearsafter, • Bonemarrow: severaldistortedcells of myeloidlineageshowingvariousabnormalities. Myeloblastsmay be increased, but below 20%. Ifhigher – itisalready leukemia, • Survival:primary MDS-9-29 mo, therapy-related – 4 to 8 mo.