Download
1 / 31
310 likes | 514 Vues
Nutrition Management in Children with Special Health Care Needs (CSHCN). Jackie Maurer MS, RD. Children with Special Health Care Needs (CSHCN) Definition:

E N D
Nutrition Management in Children with Special Health Care Needs (CSHCN) Jackie Maurer MS, RD
Children with Special Health Care Needs (CSHCN) Definition: Children with congenital or acquired conditions affecting physical/cognitive growth and development and who require more than the usual pediatric health care; also refers to children who have developmental disabilities, chronic conditions, or health related problems as well as those who are at risk for these conditions (JADA. 1995;95:809) Introduction
Introduction Nutrition Intervention • Critical aspect • Interdisciplinary • Preventive and therapeutic • Family centered • Community based • Culturally competent
Objectives • Understand basic measures of growth & development • Acquire fundamental skills in global assessment techniques • Appreciate general medical nutrition therapy for lung diseases • Experience oral supplements that promote nutrition status
GROWTH & DEVELOPMENT • Weight • Primary indicator for over-/under- nutrition • Growth chart • Reflects growth pattern • Technique • Needs to be consistent and accurate (ie no shoes, no diapers)
GROWTH & DEVELOPMENT • Height • Has slower response to nutrition changes • May indicate chronic under-nutrition if measurements continually trend down • Technique: 0-36 months - Recumbent length 2-20 years - Standing height
GROWTH & DEVELOPMENT • Head Circumference • Last indicator to be affected by undernutrition • < 3 yr old Possible nutritional insult with downtrends, accompanied by decreases in weight and height • > 3 yr old Decreases are generally not nutrition-related FOR MORE INFO... See CDC web site, http://www.cdc.gov/growthcharts, to download charts.
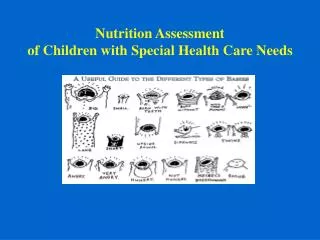
ASSESSMENT SKILLS • Subjective Global Assessment (SGA) • Simple technique for assessing nutritional status • Evaluates body fat and muscle stores • Involves visual review of physical body • May be applied by any healthcare worker • Nutrition History • Interview reveals dietary habits • Quick tool for assessing one’s ability to meet, fail, or exceed nutritional needs
Fat Stores Eye fat pad Cheek pad Tricep pinch Muscle Stores Temple Clavicle Shoulder Scapula Upper joint area Interosseus area SGA METHOD REFERENCE: Detsky, A, et al. Journal of Enteral and Parenteral Nutrition. 11:8, Jan/Feb, 1987.
http://www.eneph.com/feature_archive/nutrition/v25n4p190.htmlhttp://www.eneph.com/feature_archive/nutrition/v25n4p190.html
DIET HISTORY METHOD • What is the home life/meal pattern? • How much is consumed? • Food allergies or intolerances? • Who is present at mealtimes? • Is the child interested in eating? • Any problems with chewing or swallowing? Gagging or choking? • Are there any foods or textures that the child has difficulty with? • Does the child eat non-foods ? • Any weight change perceived? • What religious or cultural backgrounds are present?
ASTHMA & NUTRITION • Malnutrition of excess • Cycle of inactivity • Steroid induced • Potential food allergy triggers • Nutrient Medication Interactions
ASTHMA & NUTRITION • General guidelines 1. No skipping meals (Eat min 3 x day) 2. Maintain a “normal”, balanced diet and choose sensible portions 3. Lose weight, if needed 4. Avoid excessive salt, fat, sweets 5. Increase dairy or supplements 6. Exercise daily
20 minutes total 3 times per week Aerobic activity Avoid asthma triggers May lessen Exercise Induced Asthma (EIB) Tips Check local pollen, mold, spore levels. Lengthen the time between breaks while conditioning occurs. Wear scarves over mouth and nose in winter to keep heat & moisture in lungs. Warm-up to lessen chances of EIB. Do pursed lip breathing when medication is not readily available. ASTHMA & EXERCISE
ASTHMA & FOOD ALLERGIES • Food allergies - usually NOT common trigger • Occurs in <5% of asthmatics • Difficult to diagnose • Skin tests, Blood test (RAST) • Food diary, elimination diet • Symptoms • hives, itching, eczema, sneezing, coughing, swelling of throat, nasal stuffiness, vomiting, diarrhea, cramping, collapse and sometimes death
POTENTIAL FOOD ALLERGENS • Milk and dairy products • No link to increased mucus production or bronchoconstriction • Wheat • Soy • Eggs • Peanuts • Tree nuts • Fish and shellfish Chocolate • Corn • Tomatoes • Citrus fruits • Other grains • Beef • Chicken • Sulfite-containing
ASTHMA & FOOD AIDS? • Conflicting evidence that foods can prevent asthma • Of three scientific papers on asthma & omega-3 fatty acids: • 1 showed favorable results • 1 showed no results • 1 showed negative results w/ worse asthma
BPD: Bronchopulmonary Dysplasia • Nutrition Concerns • ?Prenatal undernutrition, premature growth issues • Increased caloric intake to maintain normal or catch-up growth • Suboptimal intake due to increased effort of breathing during eating and appetite suppressing medications • Delayed development of oral feeding skills
BPD & NUTRITION • Nutrition Therapy 1. Concentrate infant formula 2. Initiate adjuvant nutrition via enteral route as indicated 3. Assess feeding skills 4. Occupational therapy/feeding specialist referral
BPD & FEEDING SKILLS • Feeding Assessment • Responses to tactile input • irritability, frenzy, drowsy, staring, silent cry • Feeding position • Oral motor control • tongue retraction/protrusion, jaw excursion • Physiologic control • heart rate • Sucking, swallowing, breathing • Caregiver/infant feeding interactions
CYSTIC FIBROSIS & NUTRITION • Multifactorial risks for malnutrition • Intake • Decreased appetite • Decreased volume consumed • Physical/mechanical/mental inability to meet nutritional needs orally • Output • Increased energy output to meet cost of breathing and coughing, higher during pulmonary exacerbations. • Malabsorption
CF & NUTRITION • Basic Nutrition Guidelines 1. High calorie diet (moderate fat) 2. Snacks 2-3 times/day 3. Salt repletion, especially with sweating 4. Pancreatic enzymes • Fat soluble vitamins in water miscible form (ADEK) • Oral Supplementation • Calorically dense • Sample tasting
Childhood Obesity • DEFINITION: BMI Percentiles (2 to 20 y.o.) • 85-95th %ile = at risk • >95th%ile Overweight • Associated risks: • Hyperlipidemia, glucose intolerance, hepatic steatosis, cholelithiasis, early maturation. hypertension, sleep apnea
Childhood Obesity - Factors • Familial influence • Fat parent = fat child • Model: eating & activity • Physical Inactivity • TV • Cuts in PE class • Heredity • Fatness • regional fat distribution • response to overfeeding
Childhood Obesity - Management CDC.org
Childhood Obesity – Treatment • Physical Activity • Diet Management • Controlled weight gain • Behavior Modification
Dietary Management • Focus on energy dense, whole foods • Limit sugar packed drinks and snacks • Watch portion sizes Over Choose