Download
1 / 1
10 likes | 114 Vues
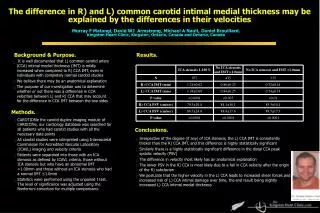
Smoking and diabetes are not associated with increased common carotid artery intimal medial thickening. Murray F Matangi, David WJ Armstrong, Michael A Nault, Daniel Brouillard. Kingston Heart Clinic, Kingston, Ontario, Canada and Ontario, Canada. Purpose. Results.

E N D
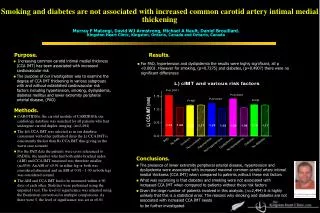
Smoking and diabetes are not associated with increased common carotid artery intimal medial thickening Murray F Matangi, David WJ Armstrong, Michael A Nault, Daniel Brouillard. Kingston Heart Clinic, Kingston, Ontario, Canada and Ontario, Canada Purpose. Results. • Increasing common carotid intimal medial thickness (CCA IMT) has been associated with increased cardiovascular risk • The purpose of our investigation was to examine the degree of CCA IMT thickening in various subgroups with and without established cardiovascular risk factors including hypertension, smoking, dyslipidemia, diabetes mellitus and lower extremity peripheral arterial disease, (PAD) • For PAD, hypertension and dyslipidemia the results were highly significant, all p <0.0001. However for smoking, (p=0.7275) and diabetes, (p=0.4907) there were no significant differences Methods. • CAROTIDfile, the carotid module of CARDIOfile our cardiology database was searched for all patients who had undergone carotid duplex imaging, (n=2,494) • The left CCA IMT was selected as in our database (consistent with other published data) the L) CCA IMT is consistently thicker than R) CCA IMT thus giving us the worst case scenario • For the PAD data the patients were cross referenced to PADfile; the number who had both ankle-brachial index (ABI) and CCA IMT measured was therefore smaller, (n=850). An ABI of <0.91 in either leg or both was considered abnormal and an ABI of 0.91 - 1.30 in both legs was considered normal. • The ABI and CCA IMT had to be measured within ± 90 days of each other. Statistics were performed using the unpaired t test. The level of significance was adjusted using the Bonferroni correction for multiple comparisons. As there were 5, the level of significance was set at <0.01 Conclusions. • The presence of lower extremity peripheral arterial disease, hypertension and dyslipidemia were associated with increased maximal common carotid artery intimal medial thickness (CCA IMT) when compared to patients without these risk factors • What was surprising is that diabetes and smoking were not associated with increased CCA IMT when compared to patients without these risk factors • Given the large number of patients involved in this analysis, (n=2,494) it is highly unlikely that this is a statistical error. The reasons why smoking and diabetes are not associated with increased CCA IMT needs • to be further investigated