Download
1 / 5
50 likes | 264 Vues
Diagnosing and Staging Asthma*. Cyril Grum, M.D. Department of Internal Medicine. *Based on the University of Michigan Guidelines for Clinic Care and the National Asthma Education and Prevention Progam (NAEPP) 2002 Update. First, make the correct diagnosis.

E N D
Diagnosing and Staging Asthma* Cyril Grum, M.D. Department of Internal Medicine *Based on the University of Michigan Guidelines for Clinic Care and the National Asthma Education and Prevention Progam (NAEPP) 2002 Update
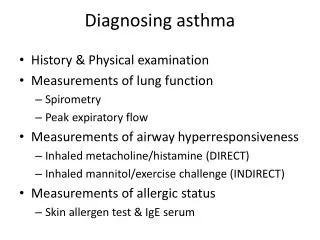
First, make the correct diagnosis • episodic symptoms of airway obstruction present • airflow obstruction present and is at least partially reversible • alternative diagnoses excluded Elements of a diagnosis of asthma:
Symptoms suggesting asthma • Cough • An attack, or recurrent attacks, of wheezing • Shortness of breath or chest tightness • Nocturnal cough • Exercise-induced cough or wheezing • Onset of symptoms after exposure to airborne allergens or other stimuli • History of persistent respiratory tract infections • Conditions associated with asthma (e.g., nasal polyps, rhinitis, atopic dermatitis, etc.)
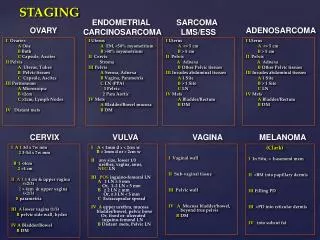
Classification by asthma severity (from MMWR March 28, 2003 / 52(RR06);1-8) Refer to document “Normal PEF tables.pdf” for normal values
Home monitoring of Peak Expiratory Flow (PEF) • Green Zone(80-100% of personal best) • “all clear” no change in therapy; if asymptomatic for a prolonged period, consider reduction in medication with monitoring. • Yellow Zone(50-80% of personal best) • “caution” suboptimal control or early exacerbation. • Red Zone(< 50% of personal best) • “alert” initiate more intense treatment , often a course of steroids.