Download
1 / 45
450 likes | 564 Vues
This conference presentation by Dr. Ethan Ellis, MD, delves into the critical role of echocardiography (Echo) in diagnosing and managing endocarditis (IE). Key topics include the ACC/AHA guidelines for Echo, comparisons between transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE), and the criteria for diagnosis based on the modified Duke criteria. The presentation emphasizes Echo's high sensitivity for identifying vegetations and associated complications, accuracy estimates, and the importance of both TTE and TEE in evaluating patient outcomes.

E N D
Echocardiography & Endocarditis Echo Imaging Conference 1/20/10 Ethan Ellis, MD
Overview • Background • Diagnosis • ACC/AHA indications for Echo • TTE versus TEE • Diagnostic Echo criteria • Echocardiographic estimation of outcome • Intracardiac complications of endocarditis • Surgical indications by Echocardiography
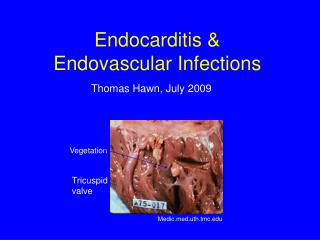
Background • Infection of endocardium • valve leaflets, congenital defects, chamber walls or chordae, prosthetic valves/conduits
Background • Infection of endocardium • valve leaflets, congenital defects, chamber walls or chordae, prosthetic valves/conduits • Diagnosis: modified Duke criteria
Background • Infection of endocardium • valve leaflets, congenital defects, chamber walls or chordae, prosthetic valves/conduits • Diagnosis: modified Duke criteria • No noninvasive technique can definitively diagnose • Echocardiography has high sensitivity for IE and intracardiac abscess • Mandatory in the diagnosis and treatment of IE • ACC/AHA 2006 guidelines on valvular heart disease include recommendations for Echo use in native and prosthetic valve IE
Goals of Echo in Possible IE • Identify, localize, and characterize masses consistent with vegetations • Identify new valvular regurgitation • Examine prosthetic valve stability • Apply criteria to judge prognosis once vegetation identified
Accuracy of TTE • Meta analysis 1984: 641 pts* • Mean sensitivity of 79% for detecting veg’s • More recently, decreased sensitivity despite tech improvements • 7 studies, 1989-1994, Mean sensitivity of 62% 4-11 • ? d/t more rigorous case selection or d/t decreased TTE scrutiny now with TEE • Limitations • Underestimates size and complexity of large veg’s • May fail to detect small veg’s (< 3 mm) *O'Brien, JT, Geiser, EA. Infective endocarditis and echocardiography. Am Heart J 1984; 108:386
Accuracy of TEE • More invasive and expensive than TTE • High sensitivity in detecting and defining valve vegetations • Same 7 studies from 1989-1994, sensitivity 92% (compared to 62%)4-11 • 5 studies w/ similar results for sensitivity also revealed high specificity for TEE and TTE (93% vs 46% sensitivity, 96% vs 95% specificity) 4,8,10-12 • ACC/AHA guidelines, main role of TEE is: • Nondiagnostic TTE • Prosthetic valve endocarditis • Assessment of complications
Diagnostic Echo criteria Characteristics of mass likely to be a vegetation: • Texture: gray scale and reflectance of myocardium
Diagnostic Echo criteria Characteristics of mass likely to be a vegetation: • Texture: gray scale and reflectance of myocardium • Location: upstream side of valve in path of jet or on prosthetic material
Diagnostic Echo criteria Characteristics of mass likely to be a vegetation: • Texture: gray scale and reflectance of myocardium • Location: upstream side of valve in path of jet or on prosthetic material • Motion: choatic and orbiting, independent of valve motion • Prolapse into upstream chamber (i.e. MV mass into LA in systole)
Diagnostic Echo criteria Characteristics of mass likely to be a vegetation: • Texture: gray scale and reflectance of myocardium • Location: upstream side of valve in path of jet or on prosthetic material • Motion: choatic and orbiting, independent of valve motion • Prolapse into upstream chamber (i.e. MV mass into LA in systole) • Shape: lobulated, amorphous • Accompanying abnormalities: • abscess, pseudoaneurysm, fistula, prosthetic dehiscence, paravalvular leak, new regurgitant lesion
Diagnostic Echo criteria Characteristics of mass unlikely to be vegetation: • Texture: reflectance of calcium or pericardium (white) • Location: outflow tract attachment, downstream surface of valve • Shape: stringy or hair-like strands with narrow attachment • Lack of accompanying turbulent flow or regurgitation
False Positives • Most common on TEE • Lambl’s excrescences • Strands on sewing rings of prosthetics • Free suture • Redundant chordae, false tendons in LV • Chiari’s remnant in RA • Chordal insertion into normal MV • All of above tend to be highly reflective with echodensity similar to pericardium or aortic root. Dense, fibrotic, non-vibratory nature
False Negatives • TTE>TEE • High sensitivity of TEE (92-94%) • Cannot definitively rule out endocarditis • Low likelihood of IE if negative TEE in intermediate probability patient • In patients at high risk for IE (prosthetic valve, unexplained bacteremia), repeat examination reasonable
Echo Estimation of Outcome • TTE: • 1991 Retrospective study. 204 pts with clinical criteria for IE.* • Clinical complications (drug failure, new CHF, embolization, surgery, death) compared to vegetation characteristics • Overall complication incidence 55% • Rates similar between native and prosthetic valves as well as between MV, TV, and AV • Size of vegetation most powerful predictor of complication • 10% if 6 mm vegetation, 50% if 11mm vegetation, almost 100% if > 16 mm • Complications more frequent with higher grades of mobility and lesion extent • Vegetation consistency did not predict complications (except for calcified lesions which had no associated complications) *Sanfilippo, AJ, Picard, MH, Newell, JB, et al. Echocardiographic assessment of patients with infectious endocarditis: Prediction of risk for complications. J Am Coll Cardiol 1991; 18:1191.
Echo Estimation of Outcome • TEE: • Observations on TTE not directly applicable to TEE since given vegetation likely to appear larger on TEE • 105 pts with IE, 1989*: • vegetation > 10 mm = increased incidence of embolization (47% v 19%, p<0.01) • Association particularly strong for MV endocarditis • Vegetation size and location did not predict other rates of complications (CHF, death) • 178 pts with IE, 2002+: • Vegetation mobility confers additional risk beyond vegetation size • Embolic incidence higher with vegetation > 15 mm (70% vs 27%) and when vegetation moderately or severely mobile (62% vs 20% compared to low mobility) • Embolic rate 83% with large and severely mobile vegetations • Observational studies suggest risk of embolism declines after institution of antibiotic therapy • Echo predictors still apply after initiation of antibiotics • Greater vegetation size and mobility still predicted late embolic events • Increase in vegetation size after antibiotic start also predicted prolonged healing phase and a higher embolic risk *Mugge, A, Daniel, WG, Frank, G, Lichtlen, PR. Echocardiography in infective endocarditis: reassessment of prognostic implications of vegetation size determined by the transthoracic and the transesophageal approach. J Am Coll Cardiol 1989; 14:631. +Di Salvo, G, Habib, G, Pergola, V, et al. Echocardiography predicts embolic events in infective endocarditis. J Am Coll Cardiol 2001; 37:1069.
Intracardiac Complications • Valvular regurgitation • Secondary infection of other valves • Leaflet perforation
Intracardiac Complications • Valvular regurgitation • Secondary infection of other valves • Leaflet perforation • Perivalvular abscess or fistula • Early invasion cellulitis (echodense thickening of perivalvular tissue) Necrosis and inflammation abscess cavity • Abscess most likely with staph aureus • Risk of fistula formation • Abscess formation increase in morbidity and mortality • TEE >TTE: 118 pts with IE, 1991, 44 with abscess at surgery/autopsy. 87% vs 28% sensitivity* • TEE still imperfect. Additional series 2007 showed TEE detecting only 48% of abscesses (21 of 44 pts)+ *Daniel, WG, Mugge, A, Martin, RP, et al. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med 1991; 324:795. +Hill, EE, Herijgers, P, Claus, P, et al. Abscess in infective endocarditis: the value of transesophageal echocardiography and outcome: a 5-year study. Am Heart J 2007; 154:923.
Right Sided Endocarditis • Tricuspid valve vegetations most common in IV drug users • Most caused by staph aureus • Infrequently, R sided endocarditis due to involvement of PV • Often diagnosed only by TEE • most literature limited to single case reports • Most reports of R sided endocarditis have used TTE • In 48 IVDU pts with suspected IE, 22 with vegetations+ • TTE and TEE equally sensitive and specific • TEE found no vegetations which were overlooked by TTE although vegetation usually better characterized by TEE +San Roman, JA, Vilacosta, I, Zamorano, JL, et al. Transesophageal echocardiography in right-sided endocarditis. J Am Coll Cardiol 1993; 21:1226.
Prosthetic Valve Endocarditis • Findings suggestive of IE in prosthetic valves: • Vegetation • perivalvular abscess and fistula formation • impaired leaflet motion • valve rocking suggesting valve dehiscence • Perivalvular regurgitation. * Must compare to prior. If no, moderate-severe suggestive of IE (not mild) • Echo evaluation can be limited by highly reflective prosthetic materials which block the passage of ultrasound • TEE has higher sensitivity than TTE (82-86% vs 36-43%)13-16 • NPV close to 100% for TEE in native valve endocarditis but not for prosthetic valves making clinical assessment especially important • According to most recent ACC/AHA guidelines, TEE should be first line diagnostic test for possible IE in prosthetic valves
Summary • Echocardiogram part of major criteria in Modified Duke Criteria • Goals to aid in diagnosis, localize vegetations, assess for complications of IE • Mass texture, location, motion, shape, and associated abnormalities important • Vegetation size and mobility correlated with embolic complications in multiple studies • TEE more sensitive than TTE. Both highly specific. • NPV high for TEE. Role for repeat imaging in high risk patients • TEE better at detecting IE complications such as abscess, fistula, and leaflet perforation • TTE = TEE in detecting R sided endocarditis with exception of PV involvement • TEE > TTE for prosthetic valve IE and should be pursued directly • ACC/AHA guidelines from 2006 include recommendations for use of TTE/TEE • Generally TTE is preferred • Class I indications TEE: nondiagnostic TTEs, better assessment of abscess/complications, prosthetic IE • Class IIA indications TEE: persistent staph bacteremia without clear source • ACC/AHA for surgical intervention (severe valve dysfunction, abscess, other penetrating lesion)
References 1. Bonow, RO, Carabello, BA, Chatterjee, K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease). J Am Coll Cardiol 2006; 48:e1. 2. Bonow, RO, Carabello, BA, Chatterjee, K, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. Circulation 2008; 118:e523. 3. Role of Echocardiography in Infective Endocarditis. UpToDate. 2010. 4. Shively, BK, Gurule, FT, Roldan, CA, et al. Diagnostic value of transesophageal compared with transthoracic echocardiography in infective endocarditis. J Am Coll Cardiol 1991; 18:391. 5. Mugge, A, Daniel, WG, Frank, G, Lichtlen, PR. Echocardiography in infective endocarditis: reassessment of prognostic implications of vegetation size determined by the transthoracic and the transesophageal approach. J Am Coll Cardiol 1989; 14:631. 6. Jaffe, WM, Morgan, DE, Pearlman, AS, Otto, CM. Infective endocarditis, 1983-1988: echocardiographic findings and factors influencing morbidity and mortality. J Am Coll Cardiol 1990; 15:1227. 7. Burger, AJ, Peart, B, Jabi, H, Touchon, RC. The role of two-dimensional echocardiology in the diagnosis of infective endocarditis [corrected] [published erratum appears in Angiology 1991 Sep;42(9):765]. Angiology 1991; 42:552. 8. Pedersen, WR, Walker, M, Olson, JD, et al. Value of transesophageal echocardiography as an adjunct to transthoracic echocardiography in evaluation of native and prosthetic valve endocarditis. Chest 1991; 100:351. 9. Daniel, WG, Mugge, A, Martin, RP, et al. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med 1991; 324:795. 10. Sochowski, RA, Chan, KL. Implication of negative results on a monoplane transesophageal echocardiographic study in patients with suspected infective endocarditis. J Am Coll Cardiol 1993; 21:216. 11. Shapiro, SM, Young, E, De Guzman, S, et al. Transesophageal echocardiography in diagnosis of infective endocarditis. Chest 1994; 105:377. 12. Birmingham, GD, Rahko, PS, Ballantyne, FD. Improved detection of infective endocarditis with transesophageal echocardiography. Am Heart J 1992; 123:774. 13. Zabalgoitia, M, Garcia, M. Pitfalls in the echo-Doppler diagnosis of prosthetic valve disorders. Echocardiography 1993; 10:203. 14. Daniel, WG, Mugge, A, Grote, J, et al. Comparison of transthoracic and transesophageal echocardiography for detection of abnormalities of prosthetic and bioprosthetic valves in the mitral and aortic positions. Am J Cardiol 1993; 71:210. 15. Alton, ME, Pasierski, TJ, Orsinelli, DA, et al. Comparison of transthoracic and transesophageal echocardiography in evaluation of 47 Starr-Edwards prosthetic valves. J Am Coll Cardiol 1992; 20:1503. 16. Roe, MT, Abramson, MA, Li, J, et al. Clinical information determines the impact of transesophageal echocardiography on the diagnosis of infective endocarditis by the Duke criteria. Am Heart J 2000; 139:945.