Download
1 / 43
500 likes | 1.58k Vues
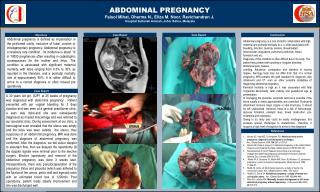
ABDOMINAL PAIN DURING PREGNANCY. s.k.s. Introduction. Abdominal pain is a very common symptom in pregnant women. It may be due to pregnancy itself e.g red degeneration in a fibroid or may arise from some concomitant lesion such as appendicitis.

E N D
Introduction • Abdominal pain is a very common symptom in pregnant women. It may be due to pregnancy itself e.g red degeneration in a fibroid or may arise from some concomitant lesion such as appendicitis. • It is convenient to divide the causes of pain due to pregnancy into those most commonly found in each of the three trimesters,though of course there is considerable overlap.
A 22 yr old para 1 with 6-8 wks gestation presents with abdominal pain. WHAT ARE YOU THINKING OF ?
The History • Colicky Pain - Localized one sided pain, no radiation, spasmodic to start with, now constant. • Mild bleeding p/v. • Some chest pain and shoulder tip pain. • Has been feeling faint. • Pregnancy test positive.
THINK ECTOPIC • VITAL SIGNS • B HCG – QUANTITATIVE • URGENT PELVIC USS • REFER/ADMIT TO HOSPITAL
ECTOPIC PREGNANCYPit falls in diagnosis • Wide variation in clinical presentation. • Pregnancy test can be negative at times of diagnosis. ( However it must have been positive at some time or another). • TV USS even at the best of hands is only 50% accurate in picking up an ectopic pregnancy. • B HCGs can double in very early ectopics. • Doubling time varies from 1.4 to 7.2 days depending on gestation.
Mx of Ectopic Pregnancy • Medical with Methotrexate with or without folinic acid. • Surgical – laparotomy and laparoscopy salpingostomy and salpingiectomy • Follow up and prognosis
First Trimester • Abortion • pregnancy in rudimentary horn • Acute salpingitis • Acute Retention of urine • Hydatidiform mole
First Trimester pain • Abortion • Pain preceeded by vaginal bleeding. • Cervix, closed (threatened abortion)or open (inevitable)..U/S.gestational sac inside uterine cavity.
First Trimester Pain • Pregnancy in rudimentary horn • pain resemble that of ectopic and usually the condition discovered during laparotomy. • If rupture occurs it usually in the midtrimester and of sudden onset with collapse.
First Trimester Pain • Acute Salpingitis • May develop up to the 10th.weeks after conception, due to gonococcal infection or infection at attempted attempted abortion • Pain felt in both iliac fossae & is continuous • There is associated tenderness,tachycardia and elevated temperature,culture of discharge may reveal pathogens
First Trimester Pain • Acute retention of urine • is usually due to enlargement of a cervical fibroid in response to pregnancy and may occur very early. • Severe lower abdominal wall, large tender bladder which may be mistaken for ovarian cyst. • Catheterisation causes immediate relief of pain.
First Trimester Pain • Hydatidiform mole • Pain in lower abdomen. • Pain due to • Overdistention of uterus • Concealed haemorrhage • Perforation • Infection • Uterine contraction for expulsion
A 22 yr old para 1 with 6-8 wks amenorrhea presents with abdominal pain The history changes: Crampy lower abdominal • Heavy bleeding p/v • Speculum examination • cx os closed • cx os open
DIAGNOSIS - ? MISCARRIAGE • Assess hemodynamic stability • Arrange pelvic ultrasound • Management depends on ultrasonographic findings. • No role of Bhcgs • Blood group, Rhesus and anti-D if necessary
SOME USS FINDINGS • An intrauterine gestational sac seen 25X30 mm in diameters. No fetus visible. • An IU gestational sac seen 20 X 20 mm in diameter. Fetal pole seen 4 mm CRL. No FH identified. • An IU gestational sac seen 20X 20 mm in diameter ,FP seen 6 mm CRL. No FH. • An IU gestational sac seen 35X35 mm in diameters low down in the cavity. FP seen . FH seen but appears slow.
THE MANAGEMENT OF MISCARRIAGE • Incomplete Abortin,Inevitable abortion,Missed abortion-Termination • ERPOC
Mid Trimester Pain • Red degeneration in a fibromyoma • Stretching of round ligament • Acute polyhydramnios • Rupture of rudimentary horn containing pregnancy • Acute retention of urine due to incarcerated RVF gravid uterus
Mid Trimester Pain • Red degeneration of fibromyoma • causes mild to severe pain. Fibroid tenderness usually present over the fibroid. • U/S usually detect the fibroid during first trimester • There may be history of menorrhagia before pregnancy..TT..conservative with analgesic
Mid Trimester Pain • Stretching of the round ligament • 10-30% of pregnancies • More in multipara • Cramp like or stabbing continuous pain and made worse with movement • Some tenderness in the lower quadrant and groin • There is no constitutional symptoms. • Reassurance and sometimes mild analgesia is required
Mid Trimester Pain • Acute polyhydramnios • Pain is due to over distention. • It can be differentiated from. pregnancy by absence of foetal heart sound.
Third Trimester Pain • Concealed haemorrhage • Severe preeclampsia • Uterine rupture • Contractions of labour • Abruptio placentae • Red degeneration of fibromyoma
Third Trimester Pain • Concealed haemorrhage • Pain is of acute onset & is severe, with considerable shock and collapse. • The abdominal mass are tense and the uterus may be larger than expected, hard tender with difficulty in palpating fetal parts. • Fetal heart is usually absent. • There may be vagina bleeding. • There may be hypertension before the event.
Third Trimester Pain • Severe Pre-eclampsia • Epigastric pain may occur & is a sign of impending eclampsia. • The characteristic signs of pre-eclampsia, hypertension, proteinuria and oedema are present • The uterus is not tender & fetal parts are palpable & FHR usually present
Third Trimester Pain • Uterine rupture • is a possibility in highly parous women & those who have scarred uterus. • Women usually feel a tearing sensation followed by constant pain. • Shock & collapse. • Vaginal bleeding is common. • Fetal parts easily felt & FHR is usually absent or distress is seen..
Third Trimester Pain • Labour pains • Prematurely or at term. I • Intermittent & gradually become stronger and more frequent. • Cervical dilatation. & effacement
A History • 22 yrs old 1st pregnancy presents with right sided abdominal pain for about 2 days. It starteds with a vague pain in the epigastrium and is now constant on the rt side. She is about 26 wks pregnant and there is no vaginal bleeding. Her 20 wk scan was “normal”.
APPENDICITIS • Most common cause of acute abdomen in pregnancy • Tenderness over McBurney’s point. • Low grade fever. • DD-Rupture ectopic pregnancy,Bilat.salphingoopheritis,Renal colic,Placental abruption,Degn.of uterine myoma.
APPENDCITIS - DIAGNOSIS • Appendix is progressively displaced upwards after 12 wks and reaches iliac crest at 24 wks. • Single most reliable symptom in pregnancy is Refferred pain • Anorexia, vomiting, rebound , guarding are not specific in pregnancy • Leucocytosis is NOT helpful.
APPENDICITIS - DIAGNOSIS • Graded compression ultrasonography accurate in 1st and 2nd trimesters , difficult in 3rd. • 98% ACCURATE.
APPENDICITIS- CONSEQUENCES • High fetal loss rate if perforation occurs (20%) • Maternal mortality • Mortality of delay • Risk of perforation highest in 3rd trimester • Premature labour esp in the 1st week after surgery
Incidental Causes of Pain • Gastro-enteritis • Pain is generalized over the abdomen and accompanied by vomiting and diarrhoea and tenesmus. • Due to irritant effect of gastric acid on peritonium. • Temperature is elevated and abdomen is tender with no rigidity. • stool analysis show organism.
Incidental causes of Pain • USG • RFT • UrineAnalysis
Incidental causes of Pain • Renal and uretric calculi • Pain may be confused as pyelitis. • pain radiates to leg and worse on movement. • Blood may be present in the urine and U/S may show stone in kidney or bladder.
Incidental causes of Pain • Cholecystitis • Right subcostal pain lower border of 9th rib, radiating to back and shoulder. • May radiate to chest . • Usually severe and lasts only for mins or hrs. • Starts at night and wakes the patient. • USG
Incidental causes of Pain • Perforation of a hollow organ • such as the stomach or duodenum, may occur with sudden pain, collapse and the rapid development of generalized peritonitis. • Usually history of peptic ulcer or gastric ulcer is present. • CXR-Gas shadow under the diaphragm.
Incidental causes of Pain • Strangulated hernia • Should be born in mind and hernial sites should be examined. • Acute Pancreatitis • the onset is sudden with severe upper abdominal pain & vomiting.usually serum amylase and urinary diastase levels elevated. • Treatment is usually symptomatic.
Incidental causes of Pain • Acute Hepatitis • May occur in hyperemesis gravidarum, in sever pre-eclampsia/eclampsia or in acute infective hepatitis. In all these conditions there is pain & tenderness over the rt.hypochondrium. • Jaundice
Incidental causes of Pain • Acute intestinal obstruction • Sometimes found in pregnancy & usually there is history of laparotomy & obstipation. • The onset is usually sudden, with vomiting. Distention & vomiting with colicky pains are typical.
Incidental causes of Pain • Torsion of ovarian cyst • may occur especially during first trimester. Pain is at first referred to one or other hypochondrium & is acute in onset usually with vomiting. • as peritonitis occur there is pain, tenderness & rigidity over the tumor. There may be some pyrexia. • TVS show the cyst. • Doppler