Download
1 / 22
410 likes | 1.33k Vues
EZ-IO in the Pediatric Patient. This presentation is only for Pediatric specific IO site location and placement. For complete IO insertion education, please refer to the website www.vidacare.com. Insertion sites. Proximal Humerus. Proximal Humerus. Proximal Tibia. Proximal Tibia.

E N D
This presentation is only for Pediatric specific IO site location and placement. For complete IO insertion education, please refer to the website www.vidacare.com T- 509
Insertion sites Proximal Humerus Proximal Humerus Proximal Tibia Proximal Tibia Distal Tibia Distal Tibia T- 509
Proximal tibia • 2 fingerbreadths below base of patella and 1 fingerbreadth medial T- 509
Proximal tibia • Pinch the sides of the tibia bone between your fingers and isolate the proximal tibia T- 509
Ability to locate accurate site on proximal tibia If TibialTuberosity cannot be palpated then find base of patella T- 509
Ability to locate accurate site on distal tibia • Place one finger directly over the medial malleolus • Move 2 fingerbreadths proximal • Palpate anterior and posterior tibia borders to confirm the flat center aspect of the bone T- 509
Proximal humerus • Should only be used in patients whose landmarks can clearly be identified surgical neck T- 509
Ability to locate accurate site on proximal humerus Elbow should remain adducted & posteriorly located Place the hand over the umbilicus for humeral positioning and safety T- 509
Ability to locate accurate site on proximal humerus • Use the thumb to palpate up the humerus until a notch/groove is felt • Insertion site is approximately 1 cm above the site. At the most prominent point T- 509
Pediatric EZ-IO insertion sites T- 509 Proximal Tibia Proximal Humerus Distal Tibia
STEP-by-step procedure T- 509
Chose appropriate insertion site • Identify the site by palpation T- 509
Primary Consider tissue depth PRIOR to bone insertion • Chose appropriate needle - 15, 25 or 45 mm • Special situations • Excessive soft tissue • Excessive muscle tissue • Edema T- 509
Prime EZ-Connect with Saline • Consider Lidocaine* if awake • Clean insertion site with antiseptic • Place needle on driver • Remove needle safety cap T- 509
Press needle set through skin until tip touches bone • At least 5 mm of the cathether must be visible T- 509
Squeeze Driver trigger • Apply gentle, steady pressure • Immediately release trigger when sudden ”give” or ”pop” is felt - indicates entry into the medullary cavity • STOP WHEN YOU FEEL THE POP T- 509
Remove Driver and stylet • Use of stabilizer is strongly recommended for pediatrics T- 509
Attach primed EZ-Connect • Flush with normal saline NO FLUSH. NO FLOW. • For patients responsive to pain,consider administering 2% lidocaine prior to flush T- 509
Confirm placement with at least 3 of 4 methods • Stability of catheter • Ability to aspirate • Physiological or pharmacologic changes • Adequate flow rate T- 509
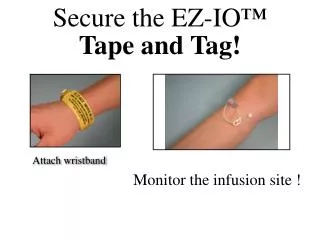
Apply EZ-IO wristband • Do not leave catheter inserted for more than 24 hours • NOTE!Monitor insertion site frequently for extravasation T- 509