Rapid Sequence Intubation
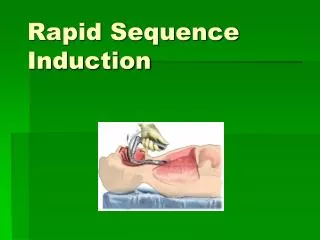
Rapid Sequence Intubation. A patient who needs intubation may be awake. Need for airway control may necessitate intubation. RSI paralyzes the patient to facilitate endotracheal intubation. Rapid Sequence Intubation. Pediatric Orotracheal Intubation. The Pediatric Airway.

Rapid Sequence Intubation
E N D
Presentation Transcript
Rapid Sequence Intubation • A patient who needs intubation may be awake. • Need for airway control may necessitate intubation. • RSI paralyzes the patient to facilitate endotracheal intubation.
The Pediatric Airway • Anatomical Differences • Smaller and more flexible than an adult • Tongue proportionately larger • Epiglottis floppy and round • Glottic opening higher and more anterior • Vocal cords slant upward, and arecloser to the base of the tongue • Narrowest part is the cricoid cartilage
Pediatric Intubation • A straight laryngoscope blade is preferred for most pediatric patients. • Selecting the appropriate tube diameter for children is critical. • ETT size (mm) = (Age in years + 16) ÷ 4 • Matching it to the diameter of the child’s smallest finger • Use non-cuffed endotracheal tubes with infants and children under the age of 8 years.
Ventilate the child © Scott Metcalfe
Prepare the equipment © Scott Metcalfe
Insert the laryngoscope © Scott Metcalfe
Visualize the child’s larynx and insert the ETT © Scott Metcalfe
Ventilate, inflate the ETT cuff (if it is a cuffed tube), and auscultate © Scott Metcalfe
Secure the tube © Scott Metcalfe
Confirm placement with an ETCO2 detector or waveform capnography © Scott Metcalfe
Reconfirm proper ETT placement © Scott Metcalfe
Ventilation of Pediatric Patients • Mask seal can be more difficult • Bag size depends on age of child • Ventilate according to current standards • Obtain chest rise and fall with each breath • Assess adequacy of ventilations by observing chest rise, listening to lung sounds, and assessing clinical improvement
Nasotracheal Intubation • “Blind” procedure without direct visualization of the vocal cords • Indications include: • Possible spinal injury • Clenched teeth • Fractured jaw, oral injuries, or recent oral surgery • Facial or airway swelling • Obesity • Arthritis preventing sniffing position
Nasotracheal Intubation • Contraindications • Suspected nasal fractures • Suspected basilar skull fractures • Significantly deviated nasal septum or other nasal obstruction • Cardiac or respiratory arrest
Nasotracheal Intubation • Advantages • The head and neck can remain in neutral position • It does not produce as much gag response and is better tolerated by the awake patient • It can be secured more easily than an orotracheal tube • The patient cannot bite the ETT
Nasotracheal Intubation • Disadvantages • More difficult and time consuming • Potentially more traumatic for patients • Tube may kink or clog more easily • Greater risk of infection • Improper placement more likely • Requires that patient be breathing
Field Extubation • Field extubation may be indicated when: • The patient is clearly able to maintain and protect his airway. • The patient is not under the influence of sedatives. • Reassessment indicates the problem that led to endotracheal intubation is resolved. • Consider the high risk of laryngospasm
Esophageal Tracheal Combitube • A dual-lumen airway • The longer, blue port (#1) is the proximal port • The shorter, clear port (#2) is the distal port, which opens at the distal end of the tube • Two inflatable cuffs • 100-mL cuff just proximal to the distal port • 15-mL cuff just distal to the proximal port
Esophageal Tracheal Combitube • Advantages • Provides alternate airway control • Insertion is rapid and easy • Does not require visualization of the larynx • Pharyngeal balloon anchors the airway • Patient may be ventilated regardless of tube placement • Significantly diminishes gastric distention • Can be used on trauma patients • Gastric contents can be suctioned
Esophageal Tracheal Combitube • Disadvantages • Suctioning tracheal secretions is impossible when the airway is in the esophagus. • Placing an endotracheal tube is very difficult with the ETC in place. • It cannot be used in conscious patients or in those with a gag reflex.
Esophageal Tracheal Combitube • Disadvantages • The cuffs can cause esophageal, tracheal, and hypopharyngeal ischemia. • It does not isolate and completely protect the trachea. • It cannot be used in patients with esophageal disease or caustic ingestions. • It cannot be used with pediatric patients.
Esophageal Tracheal Combitube Click here to view a video on ETC.
Pharyngo-Tracheal Lumen Airway • Two-tube system: • Proximal cuff seals oropharynx • Distal cuff seals either the esophagus or the trachea • Advantages • Disadvantages
Laryngeal Mask Airway • Has an inflatable distal end that is placed in the hypopharynx and then inflated • Blind insertion • Disadvantage: • Does not isolate trachea
Intubating Laryngeal Mask Airway • It is designed to facilitate endotracheal intubation. • An epiglottic elevating bar in the mask aperture elevates the epiglottis. • Tube is directed centrally and anteriorly. © LMA North America
Cobra Perilaryngeal Airway • Similar to the laryngeal mask • Supraglottic airway • “Cobra head” of the airway holds both the soft tissue and the epiglottis out of the way © Engineered Medical Systems, Inc. Indianapolis, IN
Ambu Laryngeal Mask • Supraglottic, single-use, disposable airway • Features a special curve that replicates the natural human airway anatomy © Ambu Inc. Baltimore, MD
King LT Airway • Alternative airway • Large silicone cuff that disperses pressure over a large mucosal surface area • Stabilizes the airway at the base of the tongue ©Tracey Lemons/King Systems Corporation, Indianapolis, Indiana
Foreign Body Removal Under Direct Laryngoscopy • Removing an obstructing foreign body using Magill forceps or a suction device • You should carry out basic life support maneuvers first. • If these fail to alleviate the obstruction, direct visualization of the airway for foreign body removal is indicated.
Foreign body removal with direct visualization and Magill forceps
Surgical Airways • You should use surgical airway procedures only after you have exhausted your other airway skills: • Needle cricothyrotomy • Surgical cricothyrotomy
Surgical Airways • Indications • Massive facial or neck trauma • Total upper airway obstruction • Contraindications • Inability to identify anatomical landmarks • Crush injury to the larynx • Tracheal transection • Underlying anatomical abnormalities
Needle Cricothyrotomy • Transtracheal jet insufflation is required • Complications: • Barotrauma from overinflation • Excessive bleeding due to improper catheter placement • Subcutaneous emphysema • Airway obstruction • Hypoventilation
Open Cricothyrotomy • It is preferred to needle cricothyrotomy when a complete obstruction prevents a glottic route for expiration. • Its greater potential complications mandate even more training and skills monitoring. • Contraindications: • Includes children under 12
Open Cricothyrotomy • Cricothyrotomy Complications: • Incorrect tube placement into a false passage • Cricoid and/or thyroid cartilage damage • Thyroid gland damage • Severe bleeding • Laryngeal nerve damage • Subcutaneous emphysema • Vocal cord damage • Infection
Stabilize larynx and make a 1–2 cm vertical skin incision over cricothyroid membrane