Download

1 / 58
690 likes | 1.24k Vues
Feeding the baby - Breastfeeding. Breastfeeding: A Public Health Priority.

E N D
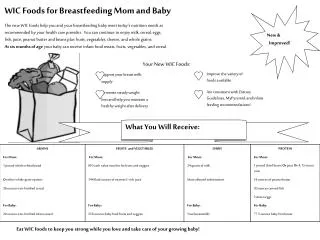
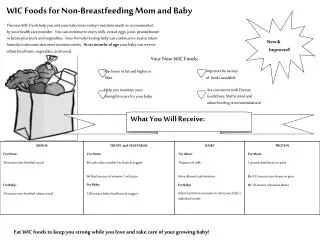
Breastfeeding: A Public Health Priority Breastfeeding has major public health benefits in reducing the incidence of certain conditions, reducing risks of infections and diseases in babies, children and women and also promoting good health in babies through transfer of antibodies from mother to baby. It also contributes to reducing children’s risks of becoming obese in the future. It is particularly important to this service because obese women are less likely to initiate and continue breastfeeding – and their children are already at increased risks of obesity.
Why Breastfeed? Breastfeeding has a number of benefits for the mother, baby and the wider family. Given your current knowledge, complete the ‘Benefits of Breastfeeding’ activity.
Why Breastfeed? - Mums Protects against ovarian and breast cancer. Protection against breast cancer is dose related – the longer the mother breastfeeds for, the better the protection Protects against weaker bones in later life Protects against hip fractures Reduced risk of Type 2 diabetes Can help promote weight loss – breastfeeding uses around 500 calories a day Can reduced stress/feelings of anxiety Promotes bonding with baby
Why Breastfeed? - Babies Protects against gastroenteritis Protects against infections including: ear, urine and chest infections Reduces risks of allergies, eczema and asthma Reduces risk of diabetes Reduces risk of sudden infant death syndrome Reduces risk of obesity Gives the baby the exact nutrients they need – no additives, preservatives or manufactured ingredients.
Why Breastfeed? - Babies Better jaw formation so lower risk of crowded teeth and better speech development– because of the action of the jaw when feeding (a narrower jaw action is used to suck from a bottle) Antibodies – babies are protected against any germs that the mother comes into contact with – once the germs are breathed in, the mother begins to produce antibodies to fight the infection. These are sent to the breasts to be included in breast milk and offer the baby immediate protection from anything the mother faces.
Why Breastfeed? - Babies Benefits that are particular to pre-term babies are that breastfeeding has been linked to better cognitive (brain) development and visual acuity as well as reducing th incidence of necrotisingenterocolitis (a serious stomach condition in premature babies)
Why Breastfeed? Benefits for families Cost and Convenience Breast milk costs very little – there is no special equipment required (although some mums will buy maternity/feeding bras, breastpads, feeding cushions etc) Formula milk costs approximately £35 per month. This doesn’t include the cost of equipment such as bottles, teats, cleaning and sterilising. Convenience – breastmilk is at the right temperature, is made on demand and available at a moment’s notice, it contains exactly right nutrients for the baby
Why Breastfeed? - Obesity Recent research into breastfeeding and obesity has suggested that: Breastfed babies were better at self-regulation of appetite – they are in control of what they eat and in later life demonstrate this Formula fed babies have faster growth patterns/weight gain in the early period which has been linked to childhood obesity Growth in last trimester and first month are key growth periods for impact on future obesity
Healthy Weight, Healthy Lives. A cross government strategy for England “Identify at risk families as early as possible and plans to promote breastfeeding as the norm for mothers.” “Whether a child is breastfed or not, and at what stage weaning begins have also shown to affect risk of excess weight later in life.”
Why Breastfeed? When talking about benefits, it is important to recognise that many of the benefits are about reducing risks. This doesn’t meant to say they will never get infections or other conditions, but they are less likely to if the mother breastfeeds/baby is breastfed. For gastroenteritis, diarrhea, formula feeding gives an increased risk because the bacteria are in the formula milk power.
Why promote breastfeeding? Considering the wealth of benefits, it may seem surprising to learn that despite those benefits, many women choose not to breastfeed. The average initiation rate for the West Midlands (percentage of babies having breastfed at within the first 48 hours) is 73% - but in many areas, the rates are much lower than that. By 6 weeks, this number has dropped to less than 50%. UK rates of breastfeeding also compare miserably with those of our European counterparts for whom rates are nearer 100% at birth.
The decline in breastfeeding Mexico 1960-100% 6 month old babies were breastfed by 1966 only 40% Chile 1960- 90% of 13 month babies breastfed by 1968 only 5% Singapore 1951 80% 3 month babies breastfed by 1971 only 5% UK steady decline from the 1950’s until late 1980’s
Why promote breastfeeding? Consider the activity “Breastfeeding – why not?”
Barriers There are a number of reasons that women may give as to why they are concerned about breastfeeding. Bottle feeding is more ‘normal’ Breasts being for pleasure Perception that bottles are more convenient Influence of family/friends Negative prior experiences Worry about feeding in public Embarrassment about feeding in public Lacking in confidence to feed Wanting baby to sleep through the night Wanting others to be involved Lack of knowledge/understanding – how it works
NHS Recommendations In 2002 the Department of Health adopted the World Health Assembly’s resolution on infant and child nutrition to: “Protect, promote and support exclusive breastfeeding for six months as a global health recommendation…. And to provide safe and appropriate complementary foods, with breastfeeding for up to 2 years and beyond.” Your role is to explain the benefits and offer the client information and support to enable them to make an informed choice.
How breastfeeding works In order to provide information and support to clients, the information in this section gives the principles of how breastfeeding works, ‘busts’ common myths and gives you the information you need to reassure and convince your clients that breastfeeding is working well – and to identify what to do if it is not. You may need to review some of the information more than once and have a look at other appropriate sources of information such as www.breastfeeding.nhs.uk .
Anatomy of the Breast • A basic knowledge of anatomy is all that you need in order to understand the principles of breastfeeding. • The diagram to the left outlines the key elements. • Milk is made to order in the alveolus by acini cells, then drawn down the ducts towards the areola and nipple when the baby sucks. There is not a huge reservoir that fills with milk and then is emptied – alveolus are constantly making milk to the demands of messages sent through the nipple by baby sucking.
Roles of Hormones • There are two hormones – Prolactin and Oxytocin – that have key roles in breastfeeding. When the baby is near, oxytocin is produced Oxytocin is also produced as a result of the baby sucking at the breast. Prolactin is only produced as a result of the baby sucking at the breast. • Prolactin is responsible for milk production. • Oxytocin is responsible for the delivery of milk
Prolactin and milk production When the baby suckles at the breast as message is sent to the brain – this makes the pituitary gland produce prolactin. The prolactin travels via the bloodstream to the breasts and the milk producing cells in the breasts (acini) begin to produce milk. The time taken for the message to travel is imperceptible as, the milk will be made and released almost as soon as the baby begins to suck at the breast. Within the acini cells, there are ‘prolactin receptors’. Recent research has suggested that these receptors need to be ‘primed’ in the early days.
Prolactin Receptors The acini cells have receptors in them and it is believed that in the first few weeks, frequent feeding enables the receptors to be ‘switched on’ by the prolactin response. Compare it to a 3 bedroom house. It has light fittings in all bedrooms – but unless there is a bulb in each fitting, you can only switch on the lights in the rooms with a bulb. Or you would need to move the bulb around. This would limit the light you could have in your house. It is believed that early, frequent feeding enables all the receptors to be ‘switched on’ so that in the future, the mother will be able to make as much milk as her growing baby needs. The ability to switch on new receptors is thought to finish at around 2 weeks after birth – so early feeding is very important for future feeding.
The prolactin receptor theory Surges of prolactin prime the receptor sites acini (milk-secreting) cell Expulsion of placenta opens receptor sites Unprimed receptor sites shut down, reducing potential for milk production prolactin receptor site
Prolactin and milk production Prolactin is at its highest at night Helps mum to go back to sleep after feeding (bottle feeding mothers don’t have that advantage) Suppresses ovulation Levels peak after the feed – getting the cells ready for the next feed Needs to be stimulated early and frequently to be effective long term Switches on the ability for all cells to make milk
Oxytocin and milk delivery When the baby suckles at the breast a message is sent to the brain – this makes the pituitary gland produce oxytocin. It can also be triggered by sight, sound and smell of the baby. The oxytocin travels via the bloodstream to the breasts and the muscular cells contract to squeeze the milk out towards the nipple. The oxytocin reflex is also referred to as the ‘let down’ reflex.
Oxytocin and milk delivery Levels are highest when baby is close to mother Stimulated by positive emotions May be inhibited by stress Induces feelings of well being After first few days is a conditioned response Works before or during a feed to make the milk flow
Who or what is FIL? Breastfeeding works on a supply and demand basis. The baby suckles and sends messages that milk is needed. The hormones respond and supply and release the milk required. The baby stops sucking and the milk stops being produced/ejected. There is also another factor in play – FIL. FIL is also known as Feedback Inhibitor of Lactation.
Feedback inhibitor of lactation [FIL] FIL is a protein that is found in the breastmilk. Whilst milk is being removed and the nipple stimulated it is inert – ie is isn’t doing anything. When the nipple stops being stimulated, or milk stops being removed, FIL begins to act within the breast to stop the acini cells making milk. Whilst the levels of FIL in the breast are high, this will stop the breast producing milk – milk that isn’t needed. When the baby suckles again and milk begins to be removed, FIL stops working to allow milk to be produced. This ensures that the breasts don’t over produce milk that isn’t needed and responds to the needs of the baby. This is a reason frequent feeding is encouraged. FIL needs to be removed to ensure continued milk production.
Early Days The first milk produced by the mum will be colostrum – this is a highly concentrated type of milk that contains a huge does of antibodies and enough nutrients to sustain the bay until the breasts begin to produce milk at day 3-5. It also contains a laxative that helps the baby get rid of the dark, sticky first poo. Colostrum is only made in very small quantities, so it is common for the baby to feed frequently in the first few days – and for the mum to think that they haven’t got enough milk. On the 3rd or 4th day, her breasts will begin to produce larger quantities of milk and will become quite full until the breasts adapt to how much milk the baby needs/wants.
Feeding Patterns In the early days it is quite common for babies to feed frequently – every hour or couple of hours – as they are developing their skills, switching on the receptors and developing patterns of feeding. They also use feeding a comfort and to be close to their mother. Consider the last 24 hours and how frequently you ate or drank something – some days you would have a set pattern, other days you may not. Babies are not so different – they enjoy comfort eating, sometimes they are thirsty – others they are feeding to satisfy hunger.
Feeding Patterns During a feed, the make up of the milk changes to meet the needs of the baby. The milk at the start of the feed is in larger quantities of lower fat, thirst quenching milk. Later in the feed, this becomes more fatty, hunger satisfying milk. Consequently, babies suck more quickly at the beginning of a feed and then settle into a slower sucking pattern, often resting and then sucking again. At the end of the feed, they must work even harder to get the small quantities of high fat milk. See the graph on the next page for a visual image of fat during a feed.
Feeding Patterns Volume of milk TIME Low-fat milk Fat globules
Feeding Cues There are a number of ways a new baby communicates that it wants to feed – often we perceive that crying is the way for it to tell us. Crying is the way a baby communicates for a number of reasons – unhappy, confused, tired, wet, dirty, etc. By recognising early feeding cues, mums can actually stop a baby from reaching the point that they are so hungry that they cry. Moving their eyes Wriggling or waving Rooting for the breast Sucking their fists, blankets etc Making murmuring noises
How breastfeeding works activity Thinking about the principles of milk production you’ve just learned, complete the Etivity – How breastfeeding works.
Helping Breastfeeding to work Following the activity, you will have come up with some things that could interfere with breastfeeding – particularly in the early days. Supplementary feeds – reduce stimulation of the breast, interfere with supply of milk – breasts think milk is not needed, interferes with positive health outcomes from breastfeeding, undermines mother’s confidence Use of a dummy – pacifies baby when it may want to feed so interferes with supply/demand, can cause confusion for baby as the sucking action is different to sucking at the breast, delays feeding cues so baby may get to crying point Using teats/bottles – can cause baby to be confused as with dummies, reduces milk transfer
Helping Breastfeeding to work To support breastfeeding, the following are useful points, particularly in the early days. Unrestricted feeding – letting baby decide how much/little they want to take, allows baby to get at the higher fat milk, less colic, ‘satisfied’ baby, baby regulates milk supply Feeding on demand/frequent feeding – help practice skills, switches on receptors, stops FIL being produced, prevents breasts becoming engorged (too full with milk) Keeping baby close – stimulates oxytocin, allows response to early feeding cues Teaching hand expression is an important skill to support breastfeeding – this will be covered later
Breastfeeding Skills Complete the activity “Breastfeeding observation”. You may find it useful to contact your local breastfeeding coordinator (Hospital or Community Trust) or a Children’s Centre locally if they run Breastfeeding Support Groups to help you to organise your breastfeeding observation.
Breastfeeding Skills From your breastfeeding observation you will have been able to identify some of the key points in how the mother was positioned and how the baby was attached during the feed. This section will cover these points in more detail and should be used alongside the video in the resources panel.
Breastfeeding Skills Position of the Mother and Baby Mother and baby must both be comfortable The mum can sit, stand or lie down – but the position she chooses should be a position she can maintain for 30 mins-60 mins comfortably. At the beginning many mums choose to sit in a chair or lie on a bed. The baby should be held close to the mother with their bodies touching. The baby’s body should be in a straight line from the top of the baby’s head down to their toes. They should be held behind their neck – their head should be free to extend The baby should be held with its nose level with the nipple
Breastfeeding Skills Positions
Breastfeeding Skills Attachment of the baby In order to effectively remove milk from the breast, the baby’s mouth needs to be attached effectively. Baby feeds from the breast not just the nipple so it important that they get a big mouthful of breast tissue Mouth will be wide open Chin should be tucked into the breast The nose should be free from the breast Baby’s cheeks should be full and round, not sucked in They use their jaw action to milk the breast More areola should be visible above the mouth than below Feeding should not be painful
Breastfeeding Skills Attachment of the baby The baby should release the breast themselves. When they do, the nipple should not be misshapen, squashed or sore If the baby is attached effectively, the nipple is drawn to the back of the mouth, beyond the hard roof of the mouth. Whilst the baby is feeding, a jaw will move and mum may see baby’s ears moving up and down Nipple shape or size shouldn’t make a difference – but those with larger nipples shouldn’t expect all of the areola to be in the baby’s mouth!
Position and Attachment Watch the video on position and attachment to consolidate your learning in this section. If you have the opportunity, practice talking through the steps of effective position and attachment with a colleague. The information in this section should give you a basic understanding of good position and attachment. If a mother is having difficulties with breastfeeding, refer them to their midwife/health visitor, breastfeeding supporter or the national breastfeeding helpline for support.
Skin to Skin Skin to skin contact is an important part of the baby’s first breastfeed – allowing mothers and babies to get to know each other and giving easy access to the breast for the baby. It is offered in most maternity units and the baby is given to the mother naked to be held against the mother’s naked chest. After birth, it helps the baby regulate its breathing and temperature, promotes the release of oxytocin in the mother and for some babies helps them to attach themselves to the breast. It can also be used later on to help sooth fractious babies, relax mum and encourage milk production.
Hand Expression Hand expression is taught to mothers in the early days to help them: Relieve breasts that are full and uncomfortable Release milk to tempt a baby who is reluctant to feed To encourage production of milk Obtain milk for a baby who cannot feed (in the neonatal unit for example) A pump is not effective in the early days because only small amounts are produced at first
Myths – I haven’t got enough milk Most women have the capacity to make enough milk for their baby – provided they feed frequently, get the position and attachment right and feed on demand and do not restrict feeds. This ensures the messages for making milk get to breasts and the breasts continue to produce milk for the baby on demand. There are only a tiny number of women (less than 3% who, for medical reasons, cannot) A baby’s tummy is very small – and babies only need very small amounts at each feed. The reason they drink more formula is that the way we feed formula milk encourages them to stretch their stomachs - they must finish that last ounce, finish the bottle etc.
Myths – I haven’t got enough milk Babies aren’t programmed to feed every 4 hours like we all believe they are – do we, as adults, only eat and drink every 4 hours? Breastmilk is also very easy to digest, which means it is digested more quickly than formula so breastfed babies may feed more frequently than formula fed babies. Babies, when they have developed their breastfeeding skills, become very adept at getting their milk quickly – so a mother may not feel they are getting enough if they are not feeding for very long. Provided the baby is getting wet and dirty nappies, is content after a feed, releases the breast themselves – these are all good signs of feeding going well
Myths – I haven’t got enough milk Tummy Size Compared to a 30ml - 90ml (1-3oz formula feed)
Myths - Sleeping Formula fed babies sleep better – some do, some don’t. Babies have only small stomachs so it is really hard for them to sleep all night without a pit-stop – they do sleep through the night eventually. Prolactin also helps breastfeeding mums (and babies) go back to sleep. It’s ok to give a breastfed baby a ‘good-night’ bottle to get a good night’s sleep – this is likely to interfere with the supply of milk by the mother, and will not guarantee that the baby will sleep. It also interferes with the health benefits of breastfeeding Formula fed babies are more content and sleep after feeds – formula takes more energy for babies to digest so they sleep whilst their bodies use energy to process that milk. Breast milk is much easier for a baby to digest