Download
1 / 8
80 likes | 187 Vues
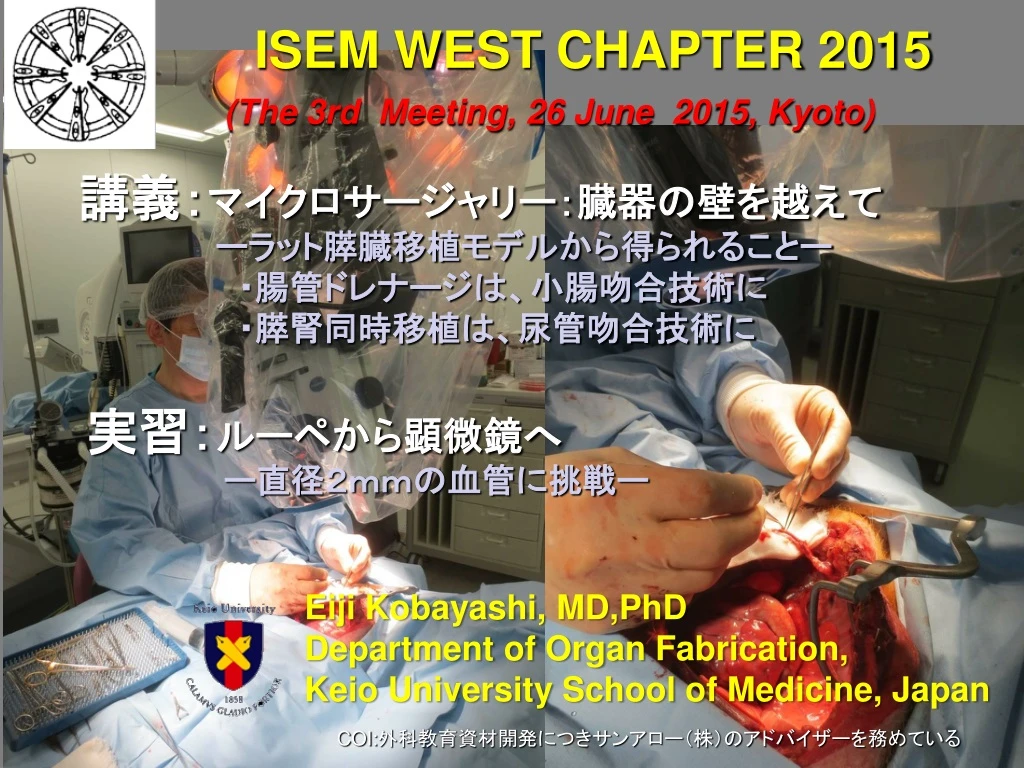
ISEM WEST CHAPTER 2015 (The 3rd Meeting, 26 June 2015, Kyoto). 講義: マイクロサージャリー:臓器の壁を越えて ーラット膵臓移植モデルから得られることー ・腸管ドレナージは、小腸吻合技術に ・膵腎同時移植は、尿管吻合技術に. 実習: ルーペから顕微鏡へ ー直径2mmの血管に挑戦ー. Eiji Kobayashi, MD,PhD Department of Organ Fabrication,

E N D
ISEM WEST CHAPTER 2015 (The 3rd Meeting, 26 June 2015, Kyoto) 講義:マイクロサージャリー:臓器の壁を越えて ーラット膵臓移植モデルから得られることー ・腸管ドレナージは、小腸吻合技術に ・膵腎同時移植は、尿管吻合技術に 実習:ルーペから顕微鏡へ ー直径2mmの血管に挑戦ー Eiji Kobayashi, MD,PhD Department of Organ Fabrication, Keio University School of Medicine, Japan COI:外科教育資材開発につきサンアロー(株)のアドバイザーを務めている
自治医科大学における小児生体肝移植プログラムにおける顕微鏡下血管吻合開始 自治医科大学における小児生体肝移植プログラムにおける顕微鏡下血管吻合開始 (2001年)
100 80 60 Survival Rate (%) 40 20 0 Year 0 1 2 3 4 5 6 Results From 2001 to 2009年 n=140
See comment in PubMed Commons belowTransplant Proc. 2010 Dec;42(10):4127-31. Living-donor liver transplantation in 126 patients with biliary atresia: single-center experience. Mizuta K1, Sanada Y, Wakiya T, Urahashi T, Umehara M, Egami S, Hishikawa S, Okada N, Kawano Y, Saito T, Hayashida M, Takahashi S, Yoshino H, Shimizu A, Takatsuka Y, Kitamura T, Kita Y, Uno T, Yoshida Y, Hyodo M, Sakuma Y, Fujiwara T, Ushijima K, Sugimoto K, Ohmori M, Ohtomo S, Sakamoto K, Nakata M, Yano T, Yamamoto H, Kobayashi E, Yasuda Y, Kawarasaki H. 1Liver Transplant Team, Jichi Medical University, Shimotsuke-shi, Tochigi-ken, 329-0498, Japan. To describe our experience with 126 consecutive living-donor liver transplantation (LDLT) procedures performed because of biliary atresia and to evaluate the optimal timing of the operation. Between May 2001 and January 2010,126 patients with biliary atresia underwent 130 LDLT procedures. Mean (SD) patient age was 3.3 (4.2) years, and body weight was 13.8 (10.7) kg. Donors included 64 fathers, 63 mothers, and 3 other individuals. The left lateral segment was the most commonly used graft (75%). Patients were divided into 3 groups according to body weight: group 1, less than 8 kg (n = 40); group 2,8 to 20 kg (n = 63); and group 3, more than 20 kg (n = 23). Medical records were reviewed retrospectively. Follow up was 4.5 (2.7) years. All group 3 donors underwent left lobectomy, and all group 1 donors underwent left lateral segmentectomy. No donors required a second operation or died. Comparison of the 3 groups demonstrated that recipient Pediatric End-Stage Liver Disease score in group 1 was highest, operative blood loss in group 2 was lowest (78 mL/kg), and operative time in group 3 was longest (1201 minutes). Hepatic artery complications occurred more frequently in group 1 (17.9%), and biliary stenosis (43.5%) and gastrointestinal perforation (8.7%) occurred more frequently in group 3. The overall patient survival rates at 1, 5, and 9 years was 98%, 97%, and 97%, respectively. Five-year patient survival rate in groups 1,2, and 3 were 92.5%, 100%, and 95.7%, respectively. Gastrointestinal perforation (n = 2) was the primary cause of death. Living-donor liver transplantation is an effective treatment of biliary atresia, with good long-term outcome. It seems that the most suitable time to perform LDLT to treat biliary atresia is when the patient weighs 8 to 20 kg
J Hepatobiliary Pancreat Sci. 2013 Oct 20. doi: 10.1002/jhbp.49. [Epub ahead of print] Risk factors and treatments for hepatic arterial complications in pediatric living donor liver transplantation. Sanada Y, Wakiya T, Hishikawa S, Hirata Y, Yamada N, Okada N, Ihara Y, Urahashi T, Mizuta K, Kobayashi E. Department of Transplant Surgery, Jichi Medical University, 3311-1 Yakushiji, Shimotsuke, Tochigi, 329-0498, Japan. Hepatic artery complications (HAC) are a serious complication in pediatric liver transplant recipients because its incidence is high and it can occasionally lead to graft liver failure. We herein present a retrospective analysis of our 10-year experience with pediatric living donor liver transplantation (LDLT) focusing on the risk factors and treatments for HAC. Between May 2001 and November 2011, 209 LDLTs were performed for 203 pediatric recipients. We performed the multivariate analyses to identify the factors associated with HAC and showed the therapeutic strategy and outcome for HAC. The overall incidence of HAC was 7.2%, and the graft survival of recipients with HAC was 73.3%. The multivariate analysis showed that the pediatric end-stage liver disease score (≥20), post-transplant laparotomy except for HAC treatment and extra-anatomical hepatic artery reconstruction were independent risk factors for HAC (P = 0.020, P = 0.015 and P = 0.002, respectively). Eleven surgical interventions and 13 endovascular interventions were performed for 15 recipients with HAC. The serum aspartate aminotransferase levels pre- and post-treatment for HAC were significantly higher in the surgical group than in the endovascular group (P = 0.016 and P = 0.022, respectively). It is important for recipients with risk factors to maintain strict post-transplant management to help prevent HAC and detect it in earlier stages. Endovascular intervention can be a less invasive method for treating HAC than surgical intervention, and can be performed as an early treatment.
Transplant Proc. 2009 Dec;41(10):4214-9 Living donor liver transplantation for congenital absence of the portal vein. Sanada Y1, Mizuta K, Kawano Y, Egami S, Hayashida M, Wakiya T, Mori M, Hishikawa S, Morishima K, Fujiwara T, Sakuma Y, Hyodo M, Yasuda Y, Kobayashi E, Kawarasaki H. Department of Transplant Surgery, Jichi Medical University, 3311-1, Yakushiji, Shimotsuke City, Tochigi, 329-0498, Japan. Abstract The congenital absence of the portal vein (CAPV) is a rare venous malformation in which mesenteric venous blood drains directly into the systemic circulation. Liver transplantation (OLT) may be indicated for patients with symptomatic CAPV refractory to medical treatment, especially due to hyperammonemia, portosystemic encephalopathy, hepatopulmonary syndrome, or hepatic tumors. Because portal hypertension and collateral circulation do not occur with CAPV, significant splanchnic congestion may occur when the portocaval shunt is totally clamped during portal vein (PV) reconstruction in OLT. This phenomenon results in severe bowel edema and hemodynamic instability, which negatively impact the patient's condition and postoperative recovery. We have successfully reconstructed the PV in living donor liver transplantation (LDLT) using a venous interposition graft, which was anastomosed end-to-side to the portocaval shunt by a partial side-clamp, using a patent round ligament of the liver, which was anastomosed end-to-end to the graft PV with preservation of both the portal and caval blood flows. Owing to the differences in anatomy among patients, at LDLT for CAPV liver transplant surgeons should seek to preserve both portal and caval blood flows.