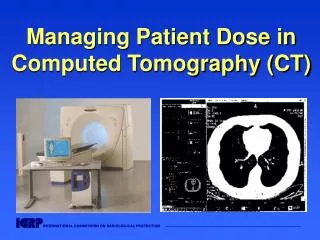
Implementing ALARA in Radiation Safety: ICRP Recommendations and New Developments
440 likes | 465 Vues
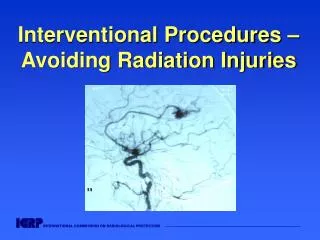
This article discusses the 10th European ALARA Network Workshop held in Prague in 2006, highlighting the experience and new developments in implementing ALARA (As Low As Reasonably Achievable) in occupational, public, and patient exposures. The article focuses on the ICRP's revised recommendations, the system of radiological protection, the linear-no-threshold hypothesis, the use of effective dose, intervention practices, optimization, and dose constraints. It also emphasizes the evolution of ALARA optimization and equity in radiation safety.

Implementing ALARA in Radiation Safety: ICRP Recommendations and New Developments
E N D
Presentation Transcript
Experience and New Developments in Implementing ALARA in Occupational, Public and Patient Eposures Optimization in ICRP Recommendations - Broadening the Process 10th European ALARA Network Workshop Prague 12 September 2006 Lars-Erik Holm Chairman of ICRP
ICRP’s 2006 Recommendations The Commission has decided to issue the revised recommendations having three primary aims in mind: • To take account of new biological and physical information and of trends in the setting of radiation safety standards; • To improve and streamline the presentation of the recommendations; and • To maintain as much stability in the recommendations as is consistent with the new scientific information.
What Is New? • There is more continuity than change! • Most recommendations will remain - because they work • and are clear. • Some recommendations are to • Be explained - because more guidance is needed; • Be added - because there has been a void; or • Differ - because understanding has evolved.
The System of Radiological Protection • Types of exposure situations; • Types of radiation exposure; • Identification of the exposed individuals; • Source-related and individual-related approaches; • The three fundamental principles of protection; • Levels of individual dose that require protective action; • Conditions for the safety of radiation sources; and • Implementation of the recommendations.
Linear-no-threshold (LNT) Hypothesis … is the basis for: • Averaging and summing of doses • The concept of effective dose • The concept of committed and collective dose • Individual dosimetry with integrating detectors • The system of keeping dose records
The System of Protection - Major Features • Maintaining the fundamental principles of radiological protection, and clarifying how they apply to sources and the individual; • Updating the weighting factors and the detriment; • Maintaining the dose limits; • Extending the concept of constraints in the source-related protection to all situations.
Summary of Radiation Risks • The nominal risk estimates are now slightly smaller than in 1990, but the risk is in the same order of magnitude as before. • The overall risk coefficient of 0.05 Sv-1 continues to be appropriate for purposes of radiological protection.
Tissue Weighting Factors , wT • Take account of - Cancer incidence - DDREF - Different populations - Lethality, quality of life, and years of life lost • Normalise to unity • Bin into 4 groups broadly reflecting relative detriments
The Use of Effective Dose, E • For compliance of constraints and dose limits to control stochastic effects • Mainly for planning in prospective situations • Not for detailed retrospective dose and risk assessments after exposure of individuals • Not for epidemiological studies
Practices and Intervention in ICRP 60 Intervention Practices Optimization Intervention Level Limit What happens below the intervention level? No further optimization? Constraints Optimization
Are Practices and Interventions Different? In both cases: • There is a maximum level of dose above which the regulator will demand action; • Optimization of protection is seen to reduce the level of dose at which action is taken; • No action to further reduce doses is taken below the optimized level of protection. CONCLUSION: There is no procedural difference
Types of Exposure Situations Replacing ‘practice’ and ‘intervention’ with three exposure situations: • Planned exposure: everyday situations involving the planned operation of practices. • Emergency exposure: unexpected situations that occur during the operation of a practice requiring urgent action. • Existing exposure: situations that already exist when a decision on control has to be taken, including natural backgroundradiation and residues from past practices.
Principles of ProtectionSOURCE RELATED OPTIMIZATION The level of protectionshould be the best under the prevailing circumstances, i.e., maximising the margin of good over harm. Optimization of protection is always constrained by a level of dose (constraint) where action is almost always warranted, and involves keeping the magnitude of individual doses, the number of people exposed, and the likelihood of incurring exposures where these are not certain to be received as low as reasonably achievable, taking into account economic and societal factors.
Optimization and Equity • Dose constraints were introduced in 1990as a means to ensure that the optimization process did not create inequity The view in RP06: • In planned situations, individual dose limits are adequate to ensure reasonable dose equity
Limits and Constraints From all regulated sources only in planned situations by THE DOSE LIMITS From a single source in all exposure situations by THE DOSE CONSTRAINTS
The Use of Dose Constraints, 1 • The basic level of protection for the most exposed individuals from a source within a type of exposure • Apply to all situations • Used prospectively at the start of the optimization process • Not a form of retrospective dose limitation • Established at national or local level, by regulator or by operator - The value selected will depend on circumstances
The Use of Dose Constraints, 2 • For planned situations: a basic level of protection, less than limits • In emergencies and in existing controllable exposure situations: a level of dose or risk where action to reduce that dose or risk is almost always warranted • An integral part of prospectively optimizing radiological protection at the source • If a relevant constraint was not complied with - Further protection options must be considered in optimization - Not necessarily a failure of protection
The Use of Dose Constraints, 3 • Numerical criteria recommended in Publication 60 and thereafter can be regarded as constraints • The values fall into three bands: 0.01-1 mSv, 1-20 mSv and 20-100 mSv • Comparison with these three bands facilitates selection of appropriate constraints for situations not addressed explicitly by ICRP
Projected Doses of 0.01 - 1 mSv/year • Planned exposures, no direct benefit to them but a benefit to society • There should be general information and environmental surveillance or assessment • Doses represent a marginal increase above natural background • Exposure of members of the public from a planned operation
Projected Doses of 1 - 20 mSv/year • Individuals receive direct benefits from the exposure situation but not necessarily from the exposure or source • Individual surveillance or dose monitoring or assessment • Individual training or information • Occupational exposure in planned situations • Radon in workplaces and homes • Countermeasures in the event of an accident, e.g., sheltering and iodine prophylaxis.
Constraints for Radon Basis: Setting a level of effective dose from radon where action would be warranted: 10 mSv per year ICRP constraints: set where action is almost always warranted: Home 600 Bq m-3 (or 500 Bq m-3 ?) Work 1500 Bq m-3(or 1200 Bq m-3 ?) National constraints: set by regulators using optimization of protection, can be below the ICRP constraints
Projected Doses of 20 - 100 mSv/year • Unusual, often extreme situations • Actions to reduce exposures would be disruptive or the source is out of control • Or, benefits from the exposure situation are commensurately high • Action to reduce exposures in an emergency • Exposure to abnormally high levels of natural background radiation
Application of Dose ConstraintsOCCUPATIONAL EXPOSURE • Individual doses in well-managed operations can be used to establish a dose constraint • Occupation should be specified in fairly broad terms - x-ray diagnostic departments, - operation of nuclear power plants, or - the maintenance of nuclear installations • Usually dose constraints set at the national or local level • Sources should be specified to avoid confusion • Constraints should ensure that dose limits are not exceeded
Application of Dose ConstraintsOCCUPATIONAL EXPOSURE IN EMERGENCY SITUATIONS • Workers could incur higher doses than in planned situations, relaxation of controls could be permitted • No dose restrictions recommended for rescue operations to prevent serious injury or catastrophic conditions • Every effort should be made to keep doses < 1000 mSv to avoid serious tissue injuries (ideally < 100 mSv) • For other immediate and urgent rescue operations dose should be kept < 100mSv • Long-term recovery operations should be treated as part of planned occupational exposure
Setting Dose Constraints • For occupational exposure in planned situations: typically set by operators or, for small companies, by regulatory authorities • For public exposure in planned situations: typically set by regulatory authorities • For patients’ comforters and carers: typically set by the medical profession
Additional Radiation Dose and Risk 0.01 – 1 mSv UNACCEPTABLE RISK 1 mSv – also public dose limit TOLERABLE RISK DOSE CONSTRAINT Optimization Protection optimized ACCEPTABLE RISK (TRIVIAL RISK)
Additional Radiation Dose and Risk 1 – 20 mSv UNACCEPTABLE RISK 20 mSv – also occupational dose limit TOLERABLE RISK DOSE CONSTRAINT Optimization Protection optimized ACCEPTABLE RISK
Additional Radiation Dose and Risk 20 – 100 mSv UNACCEPTABLE RISK 100 mSv TOLERABLE RISK DOSE CONSTRAINT Optimization Protection optimized ACCEPTABLE RISK
ICRP 2006 Recommendations The System of Radiological Protection • Emphasizes a strong radiation safety culture through a cycle of continuous review and assessment to optimize radiation doses • Optimization involves evaluating and incorporating measures that tend to lower doses to workers, the public or patients • Optimization also entails consideration of avoidance of accidents and other potential exposures
Optimization of Protection • The optimization is a forward looking iterative process aimed at preventing exposures before they occur. • Optimization is the responsibility of the operating management, subject to the requirements of the authority. • An active safety culture supports the successful application of optimization by both the operational management and by the authority.
Optimization of Protection • All aspects of optimization cannot be codified; optimization is more an obligation of means than of results. • The authority should focus on processes, procedures and judgements rather than specific outcomes. • An open dialogue must be established between the authority and the operating management to ensure a successful optimization process.
Dose to the Public: Identify Exposed Person • The system of protection uses individual dose criteria • Doses to members of public cannot be measured directly - Often not at all • Doses depend on age, location, eating habits, etc. • Thus, we must characterise an exposed individual - Dose should be representative of the more highly exposed members of the population
Formerly: The Critical Group • The concept defined in 1977 • Dose limits and constraints were applied to the mean dose in a ‘critical group’ • Dose assessment methods have evolved, e.g., probabilistic techniques • ‘Critical’ has the connotation of a crisis (never intended) • ‘Group’ is confusing (the assessed dose is to an individual)
Now: The Representative Person • Characterises an individual who is representative of the more highly exposed individuals • This ‘representative person’ replaces ‘the average member of the critical group’ • Assess prospective dose - 3 age groups may be sufficient - Deterministic or probabilistic approach - Useful to involve stakeholders
The Collective Dose • Is an instrument for optimization, for comparing radiological technologies and protection procedures. • Is not intended as a tool for epidemiologic risk assessment. It is therefore inappropriate to use it in risk projections based on epidemiological studies. • The computation of cancer deaths based on collective doses involving trivial exposures to large populations is not reasonable and should be avoided. Such a use was never intended and is an incorrect use of the collective dose.
The Collective Dose For decision-aiding, more information is often necessary, e.g. for the workforce: • Number exposed, mean dose, dose range, task-related dose, etc. • When, where, how and by whom are exposures received? For decision-making, it may be reasonable to give more weight to doses that are • Moderate or high • Received in the near future
The Optimization Process Evaluation of exposure situations to identify the need for action Optimization is a forward-looking iterative process aimed at preventing exposures before they occur. Measurement of performances Identification of protection options Selection of the best option under the prevailing circumstances Implementation of the protection option TG OPIMISATION of PROTECTION
L o c a l R e g i o n a l G l o b a l I n d i v i d u a l e x p o s u r e c h a r a c t e r i s t i c s S h o r t M e d i u m L o n g ( g e n d e r , a g e É ) t e r m t e r m t e r m Basic Structure of Dose Matrix L o c a l R e g i o n a l Group dose G l o b a l I n d i v i d u a l e x p o s u r e c h a r a c t e r i s t i c s S h o r t M e d i u m L o n g ( g e n d e r , a g e É ) t e r m t e r m t e r m TG OPIMISATION of PROTECTION
Selecting Protection Options QUANTITATIVE TOOLS Methodology and tools were developed in the 1980s to compare protection options with multi-attributes and characteristics taking into account ethical, social and economical considerations.They are still valid. ICRP warns against an application of these techniques alone. TG OPIMISATION of PROTECTION
Practical Implications OPERATIONAL MANAGEMENT • Develop and provide internal policies, priorities, rules and procedures, to • Ensure the existence of a safety culture at all levels of management and the workforce COMPETENT AUTHORITIES • Establish clear policies and processes for decision-making regarding the authorisation of proposed activities • Regulatory requirements should include the need for an active safety culture in both authority and operating management.