Download
1 / 26
260 likes | 418 Vues
Painful Facts about Pain Management. Inside Primary Care. Ming Tai-Seale, PhD, MPH Texas A&M Health Science Center Funding sources: NIMH MH01935, NIA AG15737. Co-Authors. Richard Street, Jr., PhD Texas A&M University Jane Bolin, PhD, JD, RN Texas A&M Health Science Center

E N D
Painful Facts about Pain Management Inside Primary Care Ming Tai-Seale, PhD, MPH Texas A&M Health Science Center Funding sources: NIMH MH01935, NIA AG15737
Co-Authors • Richard Street, Jr., PhD • Texas A&M University • Jane Bolin, PhD, JD, RN • Texas A&M Health Science Center • Xiaoming Bao, MS • Texas A&M Health Science Center
Introduction • Chronic pain is common among older adults • PCPs deliver most pain management • PCPs serve as “Advanced Medical Home” for elderly patients • Cognitive labor • Emotional labor
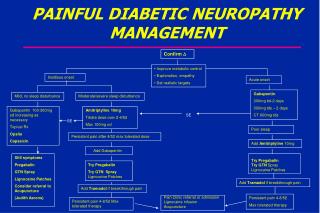
Guideline: Assessment • Assessment and documentation of • Pain location • Intensity (scale, happy/sad face…) • Onset • Duration • Variation • Rhythms and • Manner of expressing (www.Guidelines.gov)
Guideline on Treatment • Develop a written plan of care • Pharmacological management • Non-pharmacologic strategies • physical activity programs • acupuncture • patient education, and • cognitive behavioral therapy • Follow-up assessments, using same scales and measures
Realities in Practice • Time is scarce in primary care • Competing demands (Tai-Seale et al 2006) • Pressure to be “productive” and have short visits • Hot-cold empathy gap and under-treatment of pain (Loewenstein 2003) • Disparities (Bernabei et al. 1998)
Current Study Questions • What determines the probability that pain would be discussed? • What happens when pain is discussed? • How much time is spent on addressing pain? • What determines the length of time allocated to pain management?
Data • Videotapes • 385 patient visits • 35 primary care physicians • 3 types of practice settings • AMC, MCG, ICS • 1999-2000 • >2500 topics • >100 hours of recording • Patient survey • Physician survey
Mixed Method Approach • Qualitative • What happens in a visit • Was there a discussion on pain • Quantitative • How often does pain topic occur • How much time is allocated to discussing pain
Patient-Physician Dyads • Age matching • 14% age ≤10 years of each other
Visits • # of topics in a visit: • Mean = 6.5 • Median=6, Min=1, Max=12 • Average length of visit • 17.4 min • Median length of visit • 15.7 min
Descriptive Statistics • How often • 48% at least one discussion of pain • 138 contained one pain topic • 38 had two pain topics, and • 7 had 3 pain topics • How long • 3.37 min (6 sec - 15.4 min) • Patient initiation • 55%
Length of Discussion Controlled for covariates, *: p<0.05, **: p<0.01
Exemplar - Assessment Stressed out grandma, African American, SF36 pain=25 Older physician, inner city ffs solo, D: The knees bothering you? Can you expose your knees for me? (examines range of motion) Let's see, does it hurt you in here? P: No.…
Exemplar - Treatment D: Well let me tell you now, you know how bad your knees are bothering you. Use that as an indicator as to how important it is that you get the weight off them. Understand? Don't want to be falling down, hobbling like this when all you have to do is lose about 50 pounds and you'll move around much better. I'm gonna give you some tablets to take for that, you hear? … P: What did you think about the Vioxx?
Empathy gap? Emotional, cognitive labor?
Conclusions • Sociodemographics and time constraints mattered more than pain
Concordance=> better quality? • Gender concordance was the only factor in determining the probability of having a pain discussion • Length of discussion on pain was determined by time constraints and demographics • Patients with better education had longer discussions about pain • Racial concordance increases the length of discussion, but does not guarantee empathy
Implications • Standards of care • what should happen during the discussion • Primary care as “advanced medical home” • How to make it more functional • System interventions • “It’s the System!”
Are You Ready? • 50 million patients in the U.S. currently enduring chronic pain and • Another 25 million suffering from acute pain • Are you, your colleagues, and employers ready for the WAVE of patients with pain projected to flood the healthcare system when 1 in 5 individuals reach age 65 or older in the year 2011?