Renal biopsy case
Renal biopsy case. Niels Marcussen Odense University Hospital Denmark. Case history. 77-year-old male was in January 2010 operated for colon adenocarcinoma. For many years he has been treated for hypertension with beta-blockers, diuretics and alfa-blockers.

Renal biopsy case
E N D
Presentation Transcript
Renal biopsy case Niels Marcussen Odense University Hospital Denmark
Case history • 77-year-old male was in January 2010 operated for colon adenocarcinoma. • For many years he has been treated for hypertension with beta-blockers, diuretics and alfa-blockers. • In April 2010 he underwent colonoscopy which did not show any signs of recurrent disease. Prior to the colonoscopy, he was orally given sodium phosphate (OSP) bowel purgative.
Case history II • Two weeks later he was again admitted to hospital due to intestinal bleeding. At the time of admission his s-creatinine was 700 mmol/l and after rehydration 450 mmol/l. Proteinuria 1.1 g/d. No hyperphosphatemia or hypercalcemia. • A renal biopsy was done in May 2010.
Acute Phosphate Nephropathy (APhN) • Described in 2003 by S. Desmeules et al. (N Engl J M 349:1006, 2003) • Two weeks after ingesting phosphosoda a 71-year-old woman presented with malaise and elevated s-creatinine. • Analysis of the renal biopsy by X-ray dispersion spectrum: Desmeules et al. 2003
Pathogenesis of APhN • Massive phosphate intake • Diarrhea-induced hypovolemia • Decreased proximal tubular reabsorption of phosphate, especially following second dose of OSP • Hypovolemia leads to salt and water reabsorption in the tubules • Marked increase in Ca-Ph product in the distal tubular lumen Markowitz and Perazella KI 76:1027-34, 2009
Risk factors for APhN • Advanced age • Female gender • Lower body weight • Chronic renal disease • Hypertension • ACE-inhibitors, Angiotensin-receptor blockers, diuretics
Case II • 77-years-old woman with known hypertension, treated with Ca-antagonist and diuretics was admitted with increased s-creatinine (224 mmol/l). 3 months prior to admission her s-creatinine was 54 mmol/l. • The patient had 2 months prior to admission received OSP. • Urine stix was negative for blood, 1+ for protein og 2+ for leucocytes. No hypercalcemia or hyperphosphatemia. • Ultrasound normal. • Renal biopsy was performed.
Clinical outcome • Markowitz et al. 2005 and 2009: • 21 patients • 4 progressed to end-stage renal failure. • 16 declined in s-creatinine to a mean of about 210 mmol/l • 4 reached a creatinine of less then 176 mmol/l No one returned to baseline.
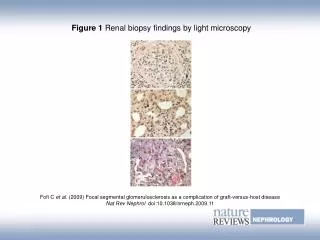
APhN, pathological changes • Acute changes (up to 3 weeks): • Acute tubular degenerative changes • Interstitial edema • Abundant tubular calcium phosphate deposits • Chronic changes (after 3 weeks): • Tubular atrophy • Interstitial fibrosis • Abundant tubular calcium phosphate deposits
Acute phosphate nephropathy • Diagnostic criteria: • AKI • Recent exposure to OSP bowel purgatives • Renal biopsy with characteristic findings • No hypercalcemia • No other known significant renal injury Markowitz & Perazella- Kidney Int 76:1027, 2009