Download
1 / 1
10 likes | 177 Vues
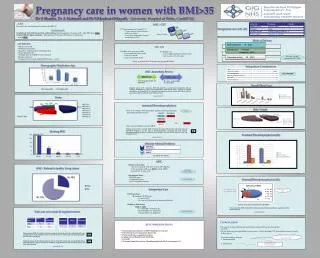
Pregnancy care in women with BMI>35 Dr S Sharma, Dr A Mahmud and Dr N Manheri-Othayoth - University Hospital of Wales, Cardiff UK. AIM To re-audit the care of pregnant women with BMI>35 STANDARDS

E N D
Pregnancy care in women with BMI>35Dr S Sharma, Dr A Mahmud and Dr N Manheri-Othayoth - University Hospital of Wales, Cardiff UK • AIM • To re-audit the care of pregnant women with BMI>35 • STANDARDS • Cardiff and Vale NHS Trust Policy and Guideline for management of women with high BMI dated 2008 • CMACE/RCOG Joint Guideline - Management of Women with Obesity in Pregnancy- March 2010 ANC - GTT Intrapartum care – IOL (19) • GTT performed in 34 cases(97.1%) - 1 case could not attend due to child care issues - 1 case note from other hospital no mention of GTT 80% GTT 2008 Mode of Delivery • METHODS • Prospective audit • Proforma developed • Duration: 12th May 2011 to 20th June 2011 • Cases identified: 36 • All Inpatients with BMI>35 were included • Results analysed • Compared to previous Audit 2008 (74 cases – 1 year) ANC - GTT For BMI >45 or previous GDM- 2 cases performed at 9 weeks- 1 case at 18 weeks- 1 case at 25 and 29 weeks For BMI 36 - 44- 2 cases performed at 12 and 14 weeks- rest mostly at 26 - 28 weeks SVD 43% C/s 42% Instrumental 15% 2008 None performed at 14 weeks (as per guidelines) Demographic Distribution Age Intrapartum Complications ANC Anaesthetic Review 16% PPH 2008 Overall Blood Loss Pregnant women with a booking BMI ≥40 should have an antenatal consultation with an obstetric anaesthetist, so that potential difficulties with venous access, regional or general anaesthesia can be identified. An anaesthetic management plan for labour and delivery should be discussed and documented in the medical records. 70% 18-30yrs 2008 55.5% 18-30yrs 2011 CMACE/RCOG Parity Antenatal Thromboprophylaxis Baby Weight • Out of 36 women 5 were prescribed aspirin or Enoxaparin as per thromboprophylaxis policy (13.8%) Primi 36% 2008 Both = • One case of 36 BMI missed h/o DVT Pregnant women with a booking BMI ≥30 should be assessed at their first antenatal visit and throughout pregnancy for the risk of thromboembolism. Antenatal and post delivery thromboprophylaxis should be considered in accordance with the RCOG Clinical Green Top Guideline No. 37. 41 Booking BMI B Postnatal Thromboprophylaxis (36) CMACE/RCOG Obstetric Medical Problems 15 out of 36 = 41.6% ANC • Review at 36 weeks: • - Out of 36 cases 31 were reviewed in ANC (86.1%) • - USG was done in 29 cases (80.5%) while EFBW was stated in 5 cases only • Intrapartum Sheet: • - Blank 14 cases- Complete 10 cases- 50% Completion 14 cases ANC - Referral to healthy living classes 78% 2008 USG 7% 2008 60% in 2008 Postnatal Thromboprophylaxis (21) Intrapartum Care 48% cases in 2008 58.3% • TEDS in labour: • - 20 cases had TEDS in all • - 2 cases of SVD • - 18 cases of C-section or Instrumental delivery • Weight on Admission: • - Only 3 cases • - 1st case BMI = 78 Repeat 83 • - 2nd case BMI = 56 Repeat 61 • - 3rd case BMI = 40 Repeat 44 Only 4 cases had clexane prescribed BD All women with a BMI ≥40 should be offered postnatal thromboprophylaxis regardless of their mode of delivery. 3 cases in 2008 Folic acid and vitamin D supplementation CMACE/RCOG CONCLUSION RECOMMENDATIONS • 36 cases in 38 days indicates the proportion of large BMI women that deliver at UHW • We are following trust guidelines in most cases i.e. Early booking GTT, Anaesthesia review, 36 week follow-up, etc. • We still are falling short on: • 1. Documentation • 2. Assessment • Knowledge and awareness of BMI Guideline is essential • Documentation on Intrapartum sheet vital • Friday teaching – as guideline updates • Update current Health Board Guideline • Re-Audit • Wide implementation of new Thromboprophylaxis Risk Assessment tool Women with a BMI ≥30 wishing to become pregnant should be advised to take 5mg folic acid supplementation daily, starting at least one month before conception and continuing during the first trimester of pregnancy. B B Referral to healthy living/weight loss Vitamin D & Folic Acid Intrapartum sheets Health professionals should take particular care to check that women with a booking BMI ≥30 are following advice to take 10 micrograms Vitamin D supplementation daily during pregnancy and while breastfeeding. 32 C Thromboprophylaxis Weight on Admission 36 week USG CMACE/RCOG