Spinal Anesthesia
Spinal Anesthesia. Vincent Conte, MD Associate Clinical Professor Nurse Anesthesia Program FIU College of Nursing. Spinal Anesthesia. This presentation will be divided into two sections: ANATOMY & PHYSIOLOGY PROCEDURE & TECHNIQUE. Spinal Anesthesia.

Spinal Anesthesia
E N D
Presentation Transcript
Spinal Anesthesia Vincent Conte, MD Associate Clinical Professor Nurse Anesthesia Program FIU College of Nursing
Spinal Anesthesia • This presentation will be divided into two sections: • ANATOMY & PHYSIOLOGY • PROCEDURE & TECHNIQUE
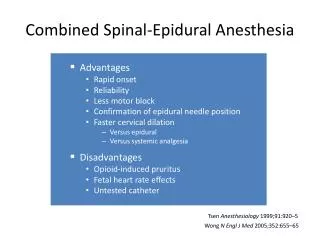
Spinal Anesthesia • Spinal, Epidural and Caudal block are also referred to by several other terms: • NEURAXIAL Anesthesia (Nerve Axis Blockade) • CONDUCTION Anesthesia (Nerve Conduction Blockade)
Spinal Anesthesia • Back to the basics: Cervical (7) Thoracic (12) Lumbar (5) Sacrum/Coccyx
Spinal Anesthesia • Boundary of Spinal CORD: Foramen Magnum to L1 • Boundary of Spinal CANAL: Foramen Magnum to Sacral Hiatus • Beyond L1: The Cauda Equina
Spinal Anesthesia • Review of Ligaments, Membranes & Spaces: (from skin in) 1) Supraspinous Ligament 2) Interspinous Ligament 3) Ligamentum Flavum 4) Epidural Space (potential) 5) Dura 6) Arachnoid 7) Sub-arachnoid space (our target) 8) Pia Mater
Spinal Anesthesia • Anatomic Landmarks to perform a Spinal Anesthetic: Bilateral Iliac Crests Body of L4 Vertebra (which should correspond to the position of a line drawn between the tops of both Iliac crests)
Spinal Anesthesia • An IMPORTANT point: When you perform your spinal anesthetic at L4-L5 or L5-S1 or L3-L4, you are injecting into the Cauda Equina and NOT any where near the actual Spinal Cord so there is no danger of damaging the spinal cord itself.
Spinal Anesthesia • (NEW STUFF): • CSF total volume between brain and spinal cord: 150cc (between 30-50cc in the Spinal Cord at any given time) • The pH of the CSF is approx. 7.32 • It is secreted by EPENDYMAL cells of the Choroid Plexus within the ventricular system at a rate of 30cc/hr • Your entire volume of CSF is replaced once every 3-4 hours
Spinal Anesthesia • NEUROANATOMY: (start at the top!) • The area of the brain that is primarily responsible for receiving painful stimuli is the “Postcentral Gyrus’ of the Parietal lobe • The area responsible for motor function and movement away from painful stimuli is the “Precentral Gyrus” of the Parietal lobe
Spinal Anesthesia • The Spinal Cord: • Extends to L1 and continues as the Filum Terminally ending at the first segment of the coccyx. • 31 (Thirty one) pairs of spinal nerves carry motor and sensory information: Cervical (8), Thoracic (12), Lumbar (5), Sacral (5) and Coccygeal (1)
Spinal Anesthesia • The spinal cord is made up of Gray and White matter • The Gray matter is composed of Neuronal cells and unmyelinated fibers. A large number of Interneurons are found in the Gray matter • The white matter contains the various tracts, both ascending and descending, with the dorsal white matter containing the ascending sensory tracts and the lateral and ventral white matter containing the descending motor tracts
Spinal Anesthesia • The nerve roots that exit the Spinal cord are divided into to two: DORSAL ROOT: carries all afferent signals heading INTO the spinal cord and brain VENTRAL ROOT: carries all efferent signals heading out to the periphery • They fuse together to form the main nerve root that exists the spinal cord at that particular level
Spinal Anesthesia • IMPORTANT: The NERVE ROOT is the primary site of action of the Local Anesthetics, both with Spinals AND Epidurals. The only difference is WHERE the root is being anesthetized, either Subarachnoid or in the Epidural space
Spinal Anesthesia • To tie it all together: A stimulus is generated and travels through a peripheral nerve back through the DORSAL root and synapses with several neurons in the gray matter and from there it goes two ways: • Up to the brain via tracts in the white matter • Back out peripherally through the VENTRAL root to muscles to cause you to withdraw from the pain
Spinal Anesthesia • Then, via the tracts in the white matter of the spinal cord, it travels via several other nerves and ends up in the Postcentral gyrus and pain is perceived • Then if further action is needed to withdraw from the pain, an impulse is generated in the Precentral gyrus, or motor center, travels DOWN the tracts in the spinal cord, synapses again in the gray matter and goes out through the VENTRAL root to the peripheral site of a muscle to cause movement
Spinal Anesthesia • Shortly after leaving the spinal cord, the meningeal coverings of the peripheral nerves merge with the connective tissue layers that cover the peripheral nerves • This becomes the Epineurium • The bundles of nerves within a peripheral nerve are covered individually by the Perineurium
Spinal Anesthesia • The nerves are further divided into the “Mantle” which is the periphery of the nerve and the “core” which is the center portion of the nerve • Each nerve bundle is further divided into the various TYPES of nerve fibers with the smallest on the periphery and the larger in the center.
Spinal Anesthesia • That is why as a nerve is anesthetized, the order of block is: Sympathetic/Parasympathetic – small fibers (C fibers; B fibers, preganglionic; afferent & efferent) Sensory – small & middle intermediate diameter fibers (C, A-delta and A-Beta; afferent & efferent) Motor – large, thick diameter fibers (A alpha, efferent) (A beta, afferent & efferent) (A gamma, efferent)
Spinal Anesthesia • The Peripheral nervous system is divided into the SOMATIC and AUTONOMIC • The Somatic system contains sensory neurons for control of skin, muscles and joint movement • Somatic motor fibers arise from the motor neurons in the ventral horn, their axons exiting the spinal cord via the Ventral root • A few centimeters out the somatic motor fibers join with incoming sensory fibers to form a mixed nerve root which eventually becomes one or many peripheral nerves
Spinal Anesthesia • So the SOMATIC system contains: INCOMING (afferent) sensory neurons for pain, proprioception, pressure, touch, etc. OUTGOING (efferent) motor fibers to skeletal muscles for movement, both reflexive and purposeful
Spinal Anesthesia • The AUTONOMIC nervous system is the other branch of the peripheral nervous system and is divided into two parts: SYMPATHETIC – (stimulating) PARASYMPATHETIC – (relaxing)
Spinal Anesthesia • The SYMPATHETIC system differs from the PARASYMPATHETIC in many ways but one of the primary differences is where the preganglionic nerve fibers end • With the Sympathetic system, they end in the sympathetic chain, in one of the many sympathetic ganglia • The Parasympathetic system preganglionic fibers actually end IN the organ that they innervate.
Spinal Anesthesia • The Sympathetic nerves also differ in that they originate in the intermediolateral gray matter of T1-L2 spinal cord segments • These sympathetic neurons run with the corresponding spinal nerve to a point just beyond the intervertebral foramen where they exit to join the sympathetic chain ganglia • The parasympathetic nerves only originate in the Cranial nerves or the Sacral nerves
Spinal Anesthesia • The Sympathetic nervous system has Alpha, Beta and Dopamine receptors • The primary neurotransmitters are Norepinephrine and Dopamine • The Parasympathetic nervous system has Nicotinic and Muscarinic receptors with Acetylcholine as its primary neurotransmitter
Differential Blockad • Spinal Anesthesia interrupts SENSORY, MOTOR AND SYMPATHETIC nervous system innervation • As the LA is injected, it blocks the small C fibers of the sympathetic system first and gradually diffuses into the interior of the nerve where the larger fibers are for sensory and then motor
Differential Blockade • Sympathetic nervous system blockade typically exceeds somatic (sensory) blockade by two (2) dermatomes • This actually may be a conservative estimate with Sympathetic blockade sometimes exceeding sensory blockade by as many as six (6) dermatomes • This explains why hypotension can accompany even low sensory block levels
Differential Levels • The Motor level is usually 2 dermatomes BELOW your sensory level due to the position of the motor fibers in the middle of the nerves. It takes longer for diffusion to get the LA into the nerves and as the concentration of LA decreases as the level rises, the amount of LA available for diffusion decreases consequently providing a weaker motor block
Differential Levels • This can have serious implications if you end up with a T4 sensory level and the sympathectomy is at T2 or higher • Cardiac Accelerator fibers of the sympathetic nervous system originate at T1-T4, so with a block at T4 you may loose their effect and bradycardia will result • Usually treated with Atropine; in severe cases Epinephrine is necessary to stimulate the heart rate sufficiently to maintain adequate cardiac output