Download
1 / 36
550 likes | 4.32k Vues
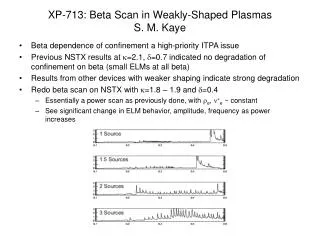
부산대학교 어린이병원 심장센터 김 시호 . Damus -Kaye- Stansel & Norwood , as procedures . Introduction. The ‘Spectrum’ needs DKS type procedures. 4 Key-Elements . Avoiding Pressure load Excessive Vol. load Minimizing PVR Maintaining optimal PA growth. Amalgamation Creation of unrestricted pathway

E N D
부산대학교 어린이병원 심장센터 김 시호 Damus-Kaye-Stansel&Norwood , as procedures.
4 Key-Elements • Avoiding • Pressure load • Excessive Vol. load • Minimizing PVR • Maintaining optimal PA growth • Amalgamation • Creation of unrestricted pathway • RV to • Aortic arch, • Descending aorta, • Coronary circulation • Establish PA flow • Perfusion strategies • Removal of interatrial septum.
Amalgamation with non-natural tissue • Homograft – Standard • Arch incision twist ↓ • Bowstring effect ↓ • ↑aggressive augmentation • LPA compression • MPA bifurcation compression • ← excessvely large proximal neoaorta • Coronary artery compromise • v shaped incision • end-to-end implantation
Amalgamation without non-natural tissue • Sano S , ATS 2009;87:178–86
Amalgamation without non-natural tissue • Mee RBB, JTCS 2000;120:875-84 • Ascending aorta implant
Amalgamation without non-natural tissue • Bowstring effect of neoaorta • Short and big neoaorta • No calcificaiton in the cuff of homograft • No growth potential • Calcification • Aneurysmal change
Amalgamation without non-natural tissue • Sung S, J Card Surg2008 Sep 12. [ahead of print]
Pulmonary Blood Flow Set-up • Systemic to pulmonary shunt (Ao-PA) • Parallel circulation • RV to PA conduit (RV-PA) • Bidirectional Cavo Pulmonary Shunt
Ao-P shunt RV-PA shunt Pulmonary Blood Flow Set-up • Good & even PA growth • Venriculotomy • ↓Ventricular function • TR • Arrhythmia • Obstruction • PA disfiguration Bad BCPS prep. • Hypoxemia Early BCPS • Limited PA growth • Diastolic pr. ↑ ↑Coronary pr. • No particular manipulations to control PVR & SVR • Good & even PA growth (?)
Perfusion strategies Imoto , JTCS 2002;122:879-82 Lim , EJTCS 2003;23:149 Tchervenkov, ATS 2000;70:1730-3
Postoperative Care All children’s Hospital symposium & “Heart week in Florida” 2007 • Hemodynamic instability (Qp, Qs) • Single ventricle • Parallel circulation • Stresses of CPB SVR ↑ • Circulatory arrest • Dynamics of neonate (Rp,Rs) • Larger shunt ; poorer systemic O2 delivery • SVR is more effect than PVR • Heart rate has a minimal effect on SaO2 • Better correlation between MVO2 and O2 delivery • Better predictor of anaerobic metabolism than BP, PP, O2 extraction rate • Optimizing SvO2 improves “complication free” survival • O2 delivery at 6 postop. hrs. - unrelated Qp/Qs • Qp/Qs = 1
Postoperative Care Advances • Routine use of VAD. Ungerleider, MD, • Increasing cardiac output during assist increase cerebral O2delivery and metabolism translate into improved neurologic outcome • Overall hospital survival – 87 % ( 95%. Lately) • Practical use of Phenoxybenzamine.Van Arsdell, MD, • Irreversible α-1 and α -2 adrenergic receptor blocker • Profound systemic vasodilator • Optimization of systemic CO by maximal dilation of systemic circulation • Prevent the acute, unexpected increases in SVR • Diminish myocardial O2consumption • Manipulate the Qs side of the Qp:Qs balance
Postoperative Care Advances Guzzetta, Anesth Analg 2007;105:312-5 Elevations in PVR Control PVR Control SVR Shunt size-doesn’t matter Tweddell, ATS 1999;67:165
Postoperative Care Example: A patient POD#3 s/p Norwood, relatively stable has oxygen saturations around 80% (by pulse ox, correlating with gases). MVS from a jugular line is 60%. What is this patient's Qp:Qs? Qp80%-60% = 20 = 1 Qs 100-%-80% 20 Qp:Qs = Sat (aorta) - Sat(SVC) Sat (pulm venous) - Sat (PA)
Postop Outcomes Ao-PA .vs. RV-PA Ao-P shunt RV-PA shunt • Hospital mortality 6.1% • Phenoxybenzamin • Home monitoring program • 4th WCPCCS in Argentina, 2005 • Hospital mortality 8% (5 of 62 patients) • Sano S , ATS 2009;87:178–86
Outcomes of DKS Out of Hospital • 2 Tails of 1 Tale
Outcomes of DKS Out of Hospital • Staged approach expecting LV growth : Stall tactic • Possibility of LV growth except for Critical AS • Especially when “semi rigid structure” (MV, AV) is normal without EFE • Restrictive PFO ↑Mitral inflow
Outcomes of HLHS According to Amalgamation • Van Arsdell, JTCS 2005;130:61-5
Outcomes of HLHS According to Amalgamation Sung S, J Card Surg 2008 Sep 12. 부산대 어린이병원 심장센터
Outcomes of HLHS ImmediateHemodynamics Ao-P .vs. RV-PA • Ghanayem, ATS 2006;82:1603-10 • 48 hour postoperative hemodynamics • Contemporary comparison • Randomized study • Higher DBP with RV-PA but, do not show increased systemic oxygen delivery
Outcomes of HLHS Vent. function Ao-P .vs. RV-PA • Ballweg, JTCS 2007;134:297-303 • Echo & Cath • RV-PA (62) or Ao-P (114) • Contemporary : • 2002 ~2005 • at the time of BCPS • Cross-sectional analysis • More ventricular dysfunction in RV-PA • during the interstage time • at the time of BCPS • Afterload reduction • 80% - RV-PA • 50% - Ao-P • Do not appear to recover with unloading of ventricle c BCPS
Outcomes of HLHS PA growth Ao-P .vs. RV-PA • Ballweg, JTCS 2007;134:297-303 • Echo & Cath • RV-PA (62) or Ao-P (114) • Contemporary : • 2002 ~2005 • at the time of BCPS • Cross-sectional analysis • “tented,” or pulled forward in RV-PA • Positioning of shunt • PA size • Preferential flow to LPA • RPA stenosis in RV-PA • Long segment distortion, hypoplasia at insertion site in RV-PA
Outcomes of HLHS at BCPC Sano , ATS 2009;87:178–86 February 1998 ~ June 2007
Outcomes of HLHS at BCPC Home surveillance • All discharged patient with Ao-P shunt (not historical control ) • Daily log of wt and SaO2 at home • Contact their physician • SaO2 < 70% • acute wt loss > 30 g in 24 hours • failure to gain at least 20 g during a 3-day period.
15.8% (n = 9/57) 0% (n = 0/24) Outcomes of HLHS at BCPC Home surveillance • Plateau phase of weight gain after 150 days
Current interstage F/U protocol • Early detection of hemodynamically important lesions • Home monitoring • Early transition (Stage 2, exp, 2v repair) ; Stage 2 should be done sooner to minimize central PA distortion • Patient selection
Summary • Apply to various anatomic pathology – Spectrum • Innovative perioperative strategies increasing success on the clinical results • No significant differences in hospital mortality and the stage 1 morbidity & mortality between Ao-P & RV-PA • Results tend to improve with most strategies “over time” must be evaluated over time by rigid analysis
Outcomes of HLHS Hemodynamics , at BCPC Ao-P .vs. RV-PA • Ballweg, JTCS 2007;134:297-303 • Echo & Cath • RV-PA (62) or Ao-P (114) • Contemporary : • 2002 ~2005 • at the time of BCPS • Cross-sectional analysis