Download
1 / 5
50 likes | 195 Vues
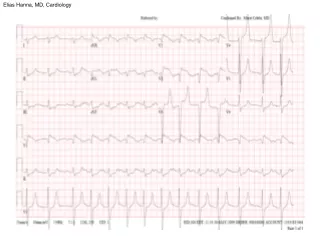
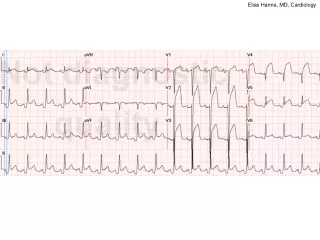
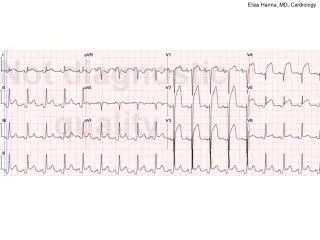
Elias Hanna, MD, Cardiology. PR depression. -Diffuse ST-segment elevation in ~all leads with ST-segment depression in aVR initially suggests pericarditis. Furthermore, PR depression in leads II, aVF, V5, V6 further suggests pericarditis.

E N D
-Diffuse ST-segment elevation in ~all leads with ST-segment depression in aVR initially suggests pericarditis. Furthermore, PR depression in leads II, aVF, V5, V6 further suggests pericarditis. -However, having pericarditis features does not necessarily imply pericarditis. In order to rule out STEMI, you should search for the 4 STEMI features and make sure none of them is present (as per next slide). -On this ECG, the morphology of the ST segment and the T wave morphology are 2 features that do not support pericarditis. ST-elevation is upwardly convex with a wide and high T wave that is fused with ST segment (see leads V2-V4).This shape is very typical of STEMI. *Also, the size of the ST elevation, > 5 mm in V2-V4 and larger than QRS in V4, is not consistent with pericarditis. ST elevation that is larger than QRS is very worrisome for STEMI.
-This pt had mid-LAD occlusion. Anterior STEMI may be associated with diffuse ST-segment elevation, particularly when a wrap-around LAD is occluded in its mid-segment leading to inferior ST-segment elevation rather than reciprocal inferior ST-segment depression *PR depression may be seen with MI and implies atrial infarction of post-MI pericarditis