Download
1 / 88
880 likes | 1.01k Vues
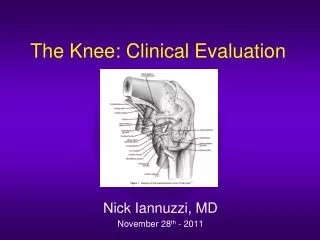
Clinical Evaluation of the Vertiginous Patient. John C. Li, M.D. Li@Dr-Li.net http://Dr-Li.net. John Li MD PA, 210 Jupiter Lakes Blvd #5105 Jupiter, FL 33458. Goals and Objectives:. Dizziness and vertigo is a very complex topic Recognize and Understand: Physiology

E N D
Clinical Evaluation of the Vertiginous Patient John C. Li, M.D. Li@Dr-Li.net http://Dr-Li.net John Li MD PA, 210 Jupiter Lakes Blvd #5105 Jupiter, FL 33458
Goals and Objectives: • Dizziness and vertigo is a very complex topic • Recognize and Understand: • Physiology • Signs and symptoms of various causes of dizziness • proper exam and tests needed for evaluation and diagnosis • Be able to educate patients using analogies • Recognize emergencies • Know when to refer
Course Mandates • Learn proper technique for evaluation of dizziness • Learn to pare down differential diagnosis by physical findings as well as symptoms • Learn canalith repositioning techniques
Definitions: • Vertigo is an abnormal sensation of movement when there is no movement actually occurring -- usually spinning sensation
Diagnosis • Diagnosis of dizziness, tinnitus and vertigo can be one of the most difficult of medical tasks. • Source of imbalance can range • Dehydration • Brain tumor. • Correct diagnosis – • Thorough history, • Physical • Tests
Why Is It So Complicated? B C D E A
So Many Differential Dx: • Salt or water imbalance, Labyrinthitis, Meniere's disease, Thyroid hormone disease, Low Blood Pressure, Sarcoidosis Autoimmune disease (Lupus, Rheumatoid arthritis), Stroke, Hi Cholesterol or triglyceride, Diabetes, Acoustic neuroma (brain tumor), Syphilis / Lymes disease, Migraines, Superior canal dehiscence, BPPV, Vestibular neuritis, Cervical vertigo, Sinusitus, Head Trauma, Concussion…..etc…
So Many Treatments • Dietary Management, Compazine, Antivert, Droperidol, Valium, Dyazide, Neptazine, Prednisone, Tumor excision, Labyrinthectomy, Streptomycin Perfusion, Vestibular Nerve Section, Vascular Loop Decompression, Endolymphatic Sac Decompression, Endolymphatic Sac Shunt, Cody Tack, Cochleosacculotomy, Canal Occlusion, Canalith Repositioning Procedure, Vestibular Rehabilitation, Accupuncture, Biofeedback, etc.
Simplify • We could teach you all the different physical findings, different tests, different treatments…. • Instead, we need orderly, way of thinking • Know the key players • Learn the physiology • Systematic algorithm • Work backwards
Diagnoses Simplified • Inner ear related (peripheral) • Other (non-inner ear)
Diagnoses • Inner ear related (peripheral) • Other (non-inner ear) • Central nervous system related (CNS) • Brain tumor • Migraine • Stroke • Systemic related • Cardiac / Syncope • Endocrine • Drugs • Psychiatric – panic attacks
Vertigo Dx. You Want to Know • Ménière’s disease / Endolymphatic Hydrops • Benign positional vertigo • Labyrinthitis / Vestibular Neuritis (15%) • Chronic vestibular weakness • Fistula /Superior Canal Dehiscence • Migraine
Definition: • Meniere’s syndrome and endolymphatic hydrops both refer to a condition of excess pressure accumulation in the inner ear.
4 Main Features • Attacks of vertigo • Fluctuating hearing loss • Tinnitus or ringing in the ears (usually low tone roaring) • Aural fullness (pressure sensation in the ears)
Physiology: Hydrops • There are two fluids that fill the chambers of the inner ear. Too much endolymph pressure will stretch these nerve-filled membranes
Increased Pressure May Be Caused by Several Disorders • Inner ear inflammation or infection or Trauma: • Autoimmune disease (Lupus, Rheumatoid dz) • Syphilis • Allergy • Metabolic / Endocrine • High Cholesterol or Triglycerides • Thyroid disease • Diabetes • Idiopathic 20
Workup of Meniere’s • History & Physical • Otoscopy Normal • Imaging: Normal • CT / MRI / MRA / MRV • Blood Tests: Normal • Audiology: • Hearing: Audiogram: Low freq SNHL • Tympanogram: Normal • Ecog : Abormal – Increased SP/AP ratio • VNG: Abormal -- RVR
Standard Treatment Options • Dietary Management • Medical Treatment • Antivert • Dyazide • Steroids • Meniett • Surgical Treatment
Dietary Management i.e. Avoid: • Foods with high sodium content. • Caffeine and tobacco • Chocolate, excessive sweets-candy, etc. • Foods with high cholesterol or triglyceride content • Foods with high carbohydrate content
Medical Treatment of Symptoms • The goal of these medications are to mask the vertigo. • Antivert: 1 tablet every 8 hours or as needed. • Droperidol: 1-2 drops under the tongue. • Compazine: 1 rectal suppository for nausea (use when too sick for pills)
Medical Treatment of Pressure Build Up • Dyazide: l “water pill” a day in the mornings.
Steroids: • Taper as directed • Very useful in acute processes • Anti-inflammatory
Surgical Treatment: • Non-Destructive Surgery • Tympanostomy tube / Meniette’s • Transtympanic Steroids • Endolymphatic Sac Decompression • Ablative (Destructive) Surgery • Transtympanic Aminoglycosides • Vestibular Nerve Section • Labyrinthectomy
Vestibular Rehabilitation • Balance retraining is important for many reasons • Improved preparedness for impending attacks • Improved tolerances of attacks • Rehab after Destructive Surgery
PICTURE BENIGN PAROXYSMAL POSITIONAL VERTIGO John Li, M.D. 30
PICTURE 2 Introduction • BPPV most common single dx of vertigo • Underestimated • Misdiagnosed • Concomitant pathology
What is BPPV? • Definition = Vertigo (a phantom sensation of motion) elicited by specific changes in head position. • Caused by placing the affected ear downward. (Classical BPPV) • Associated with characteristic eye movements (classical nystagmus)
Dizziness Characteristics • Thrown into a spin There is a lag period. • The symptoms start very violently • Dissipate within 20 or 30 seconds. • This sensation reverses upon sitting erect again.
“Classical Nystagmus” • Parallels the symptoms. • Predominantly rotatory nystagmus , fast phase toward ground • Latency (~5 sec) • Limited duration (<20 sec)
Canalith Theory Canalith Theory
Diagnosis History Physical
PICTURE Laboratory tests • Audiogram -- May be normal. • Electronystagmography -- • Caloric test not always useful
PICTURE The Hallpike Maneuver • Standard clinical test for BPPV. • Pathognomonic • A negative test is meaningless
Treatment Options • Watch and Wait vs. • "The Canalith Repositioning Procedure"
CRP video 40
What Are The Positions? • Start. Sitting, head turned 45 degrees towards ipsilateral side. • Position 1. Supine, 20-30 degrees head hanging tilt, head turned 45 degrees towards ipsilateral side. • Position 2. Supine, 45 degrees head hanging tilt, head turned 45 degrees towards contralateral side.
What Are The Positions?(3-5) • Position 3 Lying on side with contralateral shoulder down, head turned 45 degrees below horizon towards contralateral side. • Position 4 Sitting, head turned at least 90 degrees towards contralateral side. • Position 5 Straight ahead, head tilted forward.
Pearl: BPPV • Association between BPPV and Menieres! • If one exists : then possibly the other exists
Vestibular Neuritis / Labyrinthitis • Vestibular Neuronitis, Labyrinthitis • Viral infection / inflammation of the nerve / labyrinth. • Think along the lines of Bell’s Palsy • Watch out for Ramsey Hunt Syndrome
Differences • Vestibular Neuritis • Dizziness, Vertigo • Nausea, Vomiting • Labyrinthitis • Very sick • Dizziness, Vertigo • Nausea, Vomiting • Ear Pressure /Full • Hearing loss • Tinnitus • May be bacterial • Cochlear Neuritis • Ear Pressure /Full • Hearing loss • Tinnitus
Findings • Vestibular Neuritis • Abnl neuroto exam • Unilateral Vesibular weakness on ENG • Labyrinthitis • Very sick • Abnl neuroto exam • Unilat Vesibular weakness on ENG • Abnl hearing • Abnl Audio • Cochlear Neuritis • Abnl hearing • Abnl Audio 50