Download
1 / 39
440 likes | 726 Vues
Optimal Management of the Potential Organ Donor. Andrew Bernard, MD Chair, Organ Donation and Transplant Action Council Department of Surgery Magdy Giurgis , MD Department of Surgery Grand Rounds 4-14-10. Objectives. Appreciate the organ shortage

E N D
Optimal Management of the Potential Organ Donor Andrew Bernard, MD Chair, Organ Donation and Transplant Action Council Department of Surgery MagdyGiurgis, MD Department of Surgery Grand Rounds 4-14-10
Objectives • Appreciate the organ shortage • Outline the approach to a potential organ donor • Perform a brain death exam accurately
Types of Donors • Deceased Donors • Standard Criteria Donors (SCD) • Extended Criteria Donors (ECD) • >60 yrs • >50 yrs with HTN, Cr>1.5, CVA caused death • Donation after Cardiac Death (DCD) • Living Donors • Related • Non-related Brain Dead
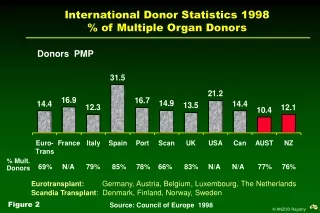
“GAP” Need for Organs Continues to Grow
Medical Complications in Failed Donors Complication Criteria % Donors Grossman Transplantation 1996; 62:1828-31
Efforts to Increase the Availability of Organs for Transplantation • Increase public awareness and improve attitudes toward donation • Increase the number of brain death donors • Increase donor consent (conversion) rates • Improve the number of organs transplanted per donor • Increase the number of ECD and DCD donors in the available pool
DO • Give everyone the chance to donate • Maximize the organs per donor • Specifically: • Optimize physiology • Slow down • Treat the family sensitively • Huddle • Help the nurses and KODA if needed
DON’T • Deny the opportunity to donate • Fail to maximize organs per donor • Specifically- • Let someone die without opportunity • Withdraw care without involving KODA • Ignore physiologic deterioration • Mention donation before a trained requestor does • Ignore the needs of the nurse, FSL or the ODC • Bring in ‘the law’
“If it’s so bad…..what next?” Response A : “The law requires that I contact KODA….” Response B : “This is Gretchen, a support specialist; she assists families who have a loved that has suffered a devastating injury.”
Deal Sensitively with Family "Talk To Me" "A negotiation is nothing more than a conversation between two people, under stress, where lives are at stake!"
Late Entry: Late afternoon, blue surgery resident, Dr. Giurgius introduced himself to GB (Gretchen, FSL), stating that he is Egyptian, as is the patient's father. Dr. Giurgius offered to help in any way if needed with communication to the father when brain death occurs.His pager number is 330-0912.
Conclusion • Give everyone a chance (70-95% would say ‘yes’)! • Max support • Slow down the family • Huddle • Move quickly to determine BD • Clinical if possible-keep it simple • If no BD, DCD?
Determining Brain Death • Clinical best if possible • 1 attending, 1 PGY-3, 1 hour between • Keep up pace (vsslowing down with family) • Confirmatory tests only if needed • M-F 8a-4p→TCD’s (Creed Pettigrew, Neurology) • Other options: • Nuclear flow • 2D angio • EEG (rarely used) • Near future → CTA • Pull up UK’s Policy @ bedside
Clinical BD Doll’s Eyes Cold Calorics 50cc, wait 1 minute, 5 minutes between Corneal Reflex
Summary • Clinical BD determination is optimal • Use the policy as a checklist • Organ Donor Intensivists • Berger • Bensadoun • Hatton • Hessel • Bernard • KODA can help
Types of Donors UNOS
Potential Organ Donor Management Supply - Demand Relationship • 105,338 patients awaiting transplant • Waiting list grows by 16% per year Waiting List % Death on List Average Wait Heart 350 days 14% Lung 788 days 12% Liver 817 days 10% Kidney 1131 days 5% HRSA