MECHANICAL PLAQUE CONTROL
1.42k likes | 3.69k Vues
MECHANICAL PLAQUE CONTROL. OBJECTIVES. Background Mechanical plaque control (a) Toothbrush (b) Dentifrice (c) Interdental cleaning aids - Dental floss - Interdental brushes - tooth pik (d) Oral irrigation. IMPORTANT CHAPTER CLINICALLY VERY RELEVANT

MECHANICAL PLAQUE CONTROL
E N D
Presentation Transcript
MECHANICAL PLAQUE CONTROL
OBJECTIVES Background Mechanical plaque control (a) Toothbrush (b) Dentifrice (c) Interdental cleaning aids - Dental floss - Interdental brushes - tooth pik (d) Oral irrigation
IMPORTANT CHAPTER CLINICALLY VERY RELEVANT REQUIREMENT FOR PATIENT TEACHING
Plaque as etiologic factor Experimental gingivitis study (1965 Löe et al. )
The cause and effect relationship between supragingival plaque and gingivitis was demonstrated by Loe et al (1965). • When plaque was allowed to accumulate, gingivitis developed within 21 days. When plaque control was initiated, the gingivitis was reversed (by means of efficient plaque control, i.e., brushing and flossing) to clinical gingival health • The removal of microbial plaque leads to cessation of gingival inflammation, and cessation of plaque control measure leads to recurrence of inflammation
The removal of plaque also decreased the rate of formation of calculus. ( Sanders , 1962) • Thus eliminating plaque is the key to prevent the occurrence of periodontal disease or halting the progression of the disease.
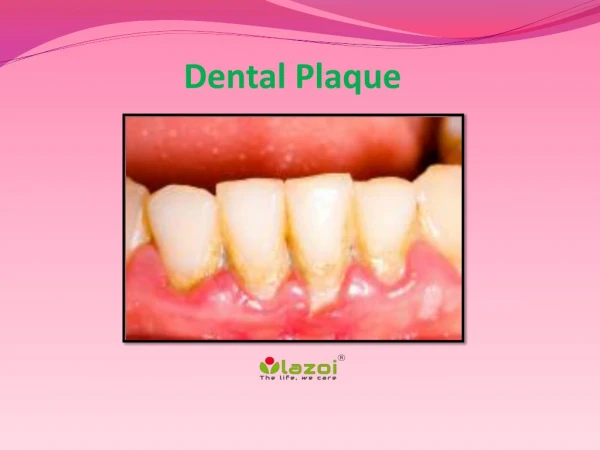
MOLAR & PREMOLAR AREAS FACIAL SURFACES OF THE MOLARS & PREMOLARS Masses of plaque first develop ( Lang,1973) PROXIMAL SURFACES OF THE ANTERIOR TEETH
PLAQUE CONTROL • Plaque control: The removal of dental plaque on a regular basis and the prevention of its accumulation on the teeth and adjacent gingival surfaces. • Position: supra- & sub-gingival plaque control • Methods: mechanical & chemical
MECHANICAL PLAQUE CONTROL • OBJECTIVE: Complete Daily Removal Of Dental Plaque With A Minimum Of Effort, Time, And Devices, Using The Simplest Methods Possible.
Self-performed • Tooth brushing • Interdental aids • Dental floss and tape • Toothpicks • Interproximal brushes • Single-tufted brush • Adjunctive aids • Dental irrigation devices • Tongue scrapers • Dentifrices
TOOTH BRUSH Toothbrush Design Methods of toothbrushing Frequency and effectiveness of toothbrushing Toothbrush wear and replacement Electric toothbrushes
The Toothbrush • First “toothbrush” -15th Century in China • First modern toothbrush - England in 1780 by William Addis – mass produced
The Toothbrush • Nylon toothbrush bristles - 1938 in USA (Du Pont) • First electric toothbrush -1960s (Broxodent) • 1987 – first rotary action electric toothbrush
The Toothbrush • Generally toothbrushes vary in size, design as well as in length and arrangements of bristleshardness. • To overcome this variation ADA given specification of toothbrushes. -------------------------------------------------
Toothbrush design American Dental Association (ADA) • Length : 1 to 1.25 inches • Width : 5/16 to 3/8 inches • Surface area : 2.54 to 3.2 cm • No. of rows : 2 to 4 rows of brushes • No. of tufts : 5 to 12 per row • No. of bristles : 80 to 85 per tuft
Natural: hog Artificial filaments: nylon Toothbrush bristles
Proportional to the square of the diameter and inversely proportional to the square of bristle length Soft brush: 0.007 inch(0.2 mm) Medium brush: 0.012 inch(0.3 mm) Hard brush: 0.014 inch(0.4 mm) Bristle hardness
short-headed brushes with straight-cut, round-ended, soft to medium nylon bristles arranged in three or four rows of tufts ARE RECOMMENDED. For most patients:
TOOTH BRUSHING TECHNIQUES Various toothbrushing technique have achieved acceptance by the dental profession. Each technique has been designed to achieve a definite goal. Depending on the individual cases, the techniques of toothbrusing may have to be altered to achieve the maximum beneficial effects.
The efficacy of brushing with regard to plaque removal is dictated by three main factors: The design of the brush The skill of the individual using the brush The frequency and duration of use 1986 Frandsen
Horizontal brushing (scrub) Leonard method (vertical) Bass method (Sulcular cleaning) Modified Bass methods Stillman methos (vibratory) Modified Stillman method (roll) Charters method Methods of cleaning with powered toothbrushes Toothbrushing methods
How to brush? • Patient is instructed to start with molar region of one arch around the opposite side than continue back around the lingual or facial surfaces of the same arch • Last surface to be brushed are occlusal. • Patient instructed to stroke each area ten time or spend 10 seconds per area then move on to next area. • Time : 2 minutes ( 30 sec per quadrant )
Charters method Bass method
Tooth Brushing • Three methods widely accepted: the modified bass method, the modified stillman method( stillman 1932), and the charters method( Carter’s 1948) . • Controlled studied evaluating the most common brushing technique have shown that no one method is superior • Recommended is Bass technique , because it emphasize sulcular placement of the bristles. • Plaque control devices should be tailored according to individual plaque control needs.
BASS OR SULCUS CLEANING METHOD Most accepted and effective method for the removal of dental plaque present adjacent to and underneath the gingival margin. • INDICATIONS • interproximal areas • cervical areas beneath the height of contour of enamel. • exposed root surfaces.
TECHNIQUE • The bristles are placed at a 45 degree angle to the gingiva and moved in small circular motions. • Strokes are repeated around 20 times,3 teeth at a time. • On the lingual aspect of the anterior teeth, the brush is pressed into the gingival sulci and proximal surfaces at a 45 angle. • The bristles are then activated. • Occlusal surfaces are cleaned by pressing the bristles firmly and then activating the bristles.
ADVANTAGES Effective method for removing plaque. Provides good gingival stimulation. DISADVANTAGES Injury to the gingival margin. Time consuming. Dexterity.
MODIFIED BASS TECHNIQUE INDICATION: As a routine oral hygiene measure Intrasulcular cleansing.
TECHINIQUE Vibratary and circular movements with sweeping motion Bristles are at 45 to the gingiva Bristles are swept over the sides of the teeth towards their occlusal surfaces in a single stroke.
ADVANTAGES EXCELLENT SULCUS CLEANING. GOOD INTER PROXIMAL AND GINGIVAL CLEANING. GOOD GINGIVAL STIMULATION DISADVATAGES DEXTERITY
MODIFIED STILLMAN’S TECHNIQUE INDICATIONS DENTAL PLAQUE REMOVAL CLEANING TOOTH SURFACES AND GINGIVAL MASSAGE . DISADVANTAGE TIME CONSUMING DAMAGE EPITHELIAL ATTACHMENT.
TECHNIQUE Bristles are pointed apically with an oblique angle to the long axis of the tooth Bristles placed on the cervical aspect of the teeth Short back and forth motion moved in a coronal direction.
CHARTER’S METHOD INDICATIONS: Persons having :- Missing papilla and exposed root surfaces. FPD and Orthodontic appliances. Periodontal surgery. Interproximal gingival recession.
TECHNIQUE A soft/medium multi-tufted tooth brush taken Bristles are placed 45 to the gingiva with bristles directed coronally. Mild vibratory strokes required with bristles ends lying interproximally.
ADVANTAGES Massage and stimulation of gingiva. DISADVANTAGES Poor removal of subgingival bacterial accumulations. Limited brush placement. Requirements in digital dexterity are high.
The Toothbrush • The use of hard toothbrush , vigorous horizontal brushing, the use of extremely abrasive dentifrices may lead to cervical abrasion of teeth and recession of the gingiva.( Jepson ,1998) • Toothbrushes need to be replaced every 3 months
The Toothbrush Soft, nylon bristle toothbrush clean effectively (when used properly), remain effective for a reasonable time , Soft bristle are more flexible and atraumatic clean beneath the gingival margin, reach farther into the proximal tooth surfaces.
EMBRASURE V-shaped spillway next to the contact area of adjacent teeth; Narrowest at the contact and widening toward the facial, lingual, and occlusal contacts
Invented in 1939. Motions: Back and forth Circular Elliptic Combinations Powered toothbrushes
Cleaning action by: Mechanical contact between the bristles and the tooth Low-frequency acoustic energy generates dynamic fluid movement and provides cleaning slightly away from the bristle tips.
INDICATIONS: Children and adolescents Children with physical or mental disabilities Hospitalized patients, including older adults who need to have their teeth cleaned by caregivers Patients with fixed orthodontic appliances.