Download

1 / 27
270 likes | 291 Vues
This presentation discusses disease-free survival rates for non-metastatic colorectal cancer cases in Iran, highlighting the increasing trend in incidence rates. The Quality Registry Network (QRN) aims to assess CRC care quality in different cancer centers for better patient outcomes.

E N D
ClinicalCancer Research Center, Iran University of Medical Sciences, Tehran, Iran rouhollahi@razi.tums.ac.ir DISEASE FREE SURVIVAL FOR NON-METASTATIC COLORECTAL CANCER CASES IN THREE REFERRAL HOSPITALS IN IRAN; INTERIM REPORT OF THE CRC QUALITY REGISTRY NETWORK (QRN-CRC) Mohammad Reza Rouhollahi; MD, PhD Candidate; Cancer Research Institute, Tehran University of Medical Sciences, Tehran, Iran
Estimated age-standardized incidence rates (World) in 2018, colorectum, both sexes, all ages
Increase Incidence Rate of CRC in Iran Through last decade (Somehow due to registration some inaccuracy in early years)
Increasing Trend for Colorectal Cancer in Golestan Province 2006-2013
Cancer Care Human Resource &Infra-structure In Iran • About one oncologist per 200 cancer patients; • More than 70 active radiotherapy Units in all parts of the country; • Many general surgery departments doing colon cancer surgery and some referral teaching colorectal surgery departments doing rectal and complicated colon cancer operations.
Our Team and Network Members • Kazem Zendehdel • Mohammad Ali Mohagheghi • SeyedHosseinYahyazadeh • FaridAzmoudehArdalan • ShamimGharagozloo • HabibollahMahmoodzadeh • Mehdi Aghili • MehrzadMirzania • AzinNahvijou • Monireh Sadat Seyyedsalehi • Hamid Reza Mirzaei • Mohammad SadeghFazeli • Mohammad Reza Keramati This presentation is on behalf of my colleagues and representatives of the cancer centers collaborating on Iran QRN-CRC.
BACKBONE • The “clinical cancer registry program (CCRP)” in Iran was first established in 2013for common cancers, particularly Breast, Colorectal and Gastric cancer. • In the CCRP dataset, NAACCR standards has been considered. • The new updates and advantages of CCRP are linkages to the databases such as: • The national identification and death registry; • National health information system; • Hospitals Information Systems The poster presented in IACR2016 annual conference Marrakesh by me and our colleagues:
BACKBONE • The new updates and advantages of CCRP are 1. Linkages to the databases such as: • The national identification and death registry; • National health information system; • Hospital Information Systems For decreasing loss to follow-up (in recognition of disease progression and death) 2. Improving the IT infra-structure with using an open-access database which has comprehensive important standards useful for registries. Recently more than 8 provinces and related 10 teaching hospitals joined to CCRP for breast and colorectal cancer.
Purpose of QRN-CRC • The aim of the Quality Registry Network (QRN) has been developing a robust model of colorectal cancer (CRC) care quality assessment based on the CCRP to determine the role of related cancer centers, particularly at first: • The referral comprehensive cancer centers; • Teaching hospitals; • Centers which are high-volume for CRC cases and surgical operations.
DEFINITION • The Institute of Medicine (IOM) defined good quality care as “providing patients with appropriate services in a technically competent manner, with good communication, shared decision making, and cultural sensitivity”, (IOM, 1999, p. 79). • Approach to evaluating “quality” is based on structure, process, and outcomes(Donabedian, 1980). • “Structural quality” refers to the ability of a health care system to meet the needs of patients or communities, • “Process quality” refers to the technical skills of health care clinicians and their interactions with patients, and • “Outcomes quality” refers to changes in patients’ health status (e.g., morbidity and mortality) What is “quality of care”? As we know, “quality of care” specially in cancer care is complex as a concept and difficult in assessment.
Political Issue! • Quality evaluation almost always makes the actors sensitive about the impacts of assessment and exists resistance against. • Even in our QRN network, there is a bit hesitancy and resistance about it and the publication of the results will be depend on committee board’s final decision.
METHODS: • The model is consisted of two interrelated parts: • A risk adjusted outcome evaluation in which risks included factors such as: • Disease prognostic factors; • Patients factors; • Treatment pathways. • Assessment and benchmarking of the most common quality indicators in CRC care. Based on the definition, model with two inter-related parts of the quality of care (outcomes and process) has been considered:
Methods (structures) • A Cancer Center of Excellence • A Colorectal Surgery Department of Excellence • A Teaching Hospital High- Volume for Colorectal Cancer Surgery • A Non-Teaching Hospital High-Volume for Colorectal Cancer Surgery Four members of the network has been selected to effects of structural quality became almost controlled or adjusted. So in interference of any disparity delivered between these level should be not mentioned the effects of structural quality. Except of 1 and 2 which are high- volume in rectal cancer surgery, in the others colon cancer operation is more common.
RISK-ADJUSTED DISEASE- FREE SURVIVAL(RADFS) • Disease Prognostic Factors: • Rectal vs. Colon Cancer • Morphology of tumor • Stage at Diagnosis • Pathologic Stage • Response to treatment and down-staging due to neoadjuvantCRTx (If it’s applicable) • Histologic Grade • CRM involvement or CRM Closed in preoperative assessment • Perineural Invasion of tumor • Lympho-vascular Invasion of tumor • Emergency at presentation (Perforation or Obstruction) • Patient Factors: • Age at diagnosis • Gender • Patients' socioeconomic status (SES) • Pre-operative status • Pre-treatment Performance • Comorbidities (Based on ASA classification) • Patients' Refusal for treatment • Treatment Pathway: (Type of regimen, cylces in CTx and fractions in CRTx) • Guideline based Neoadjuvant CRTx(If applicable) • Guideline based Neoadjuvant CTx(If applicable) • Guideline based Adjuvant CRTx • Guideline based Adjuvant CTx We should adjust the risks for DFS to compare the net effect of the surgery as the main course of treatment and finding any disparity.
Outcome Indicators • Rate of mortality 30days after surgery • Rate of mortality 180 days after surgery • Readmission and reoperation after main surgery or rate of long admission after surgery • DFS based on stage of disease • Overall survival (OS) Some important and usual outcome indicators as proxy for outcome evaluation and comparing between care (surgery) facilities
12 Quality Indicators: • Rate of good lymph node evaluation; • Rate of involved surgical margin; • Rate of perfect anastomosis and no peritoneal leak; • Rate of sphincter saving in low rectal tumors; • Rate of neglected metastatic patients underwent primary tumor surgery due to not adherence to guidelines that emphasize on an comprehensive radiologic assessment; • Rate of MRI and EUS modality and their preferences in loco-regional staging in rectal cancer; • Standardized pathology report and its elements; • Time difference between end of neoadjuvant radiotherapy and surgery in rectal cancer; • Time difference between surgery and start of adjuvant chemotherapy; • Pathologic response grade and down staging due to neoadjuvant radiotherapy in rectal cancer; • Rate of multi-disciplinary team decision-making for CRC cases. • The rate of high risk groups of stage II colon cancer received chemotherapy. Our committee board reached 12 most essential QIs for evaluating “process qualities”, based on scientific relevancy and affordability. As we know, almost all of the quality indicators is defined as a “proportion”. CLOCK OF QUALITY
MAIN CONCERN • The QIs should be mention only essentials and crucial components of CRC care; • Both of parts of the model should be comprehensive, and congruent with each other; • The model should be the customized for developing countries like Iran. Tri-angle of danger
METHODS • Determining the most relevant and affordable quality and outcome indicators by the committee board; • After we reviewed the medical records of all ascertained CRC patients who underwent surgery in fourmajor cancer centers in Iran. • All included patients or their families were called to assess the missing follow-up data up to December 2018 (about 30% percent of loss to follow-up cases before have been contacted and less than 10% remained missing after • After analyzing the data in a conducted feasibility study, main quality indicators and disease free survival (DFS) in CRC care were determined the most essential and relevant QIs in CRC care. • Final committee boards’ decision making about the results and publish them. Completeness: All cases met the inclusion criteria and their diagnoses were between Jan2013 to end of Dec2015. Timeliness: Retrospective case finding but not more than one year after patient’s diagnosis. Validity: Following the NAACCR datasets and standards, and following the guidelines
Total Numbers of Non-metastatic Patients Underwent surgery Colon vs. Rectum, Early diagnosis vs. Locally advancedTeaching vs. Non-teaching Hospitals
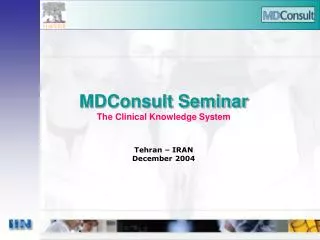
RESULTS (samples) Ongoing analysis of the data captured by the QRN network will be completed soon. In some results, we need more power so we should continue the data capturing or combine the categories of data and subgroups. P=0.98 Five-year disease free survival according to the localization of the tumor - colon vs. rectum (Incidence period 2013-2015. Follow-up date: end of 2018)
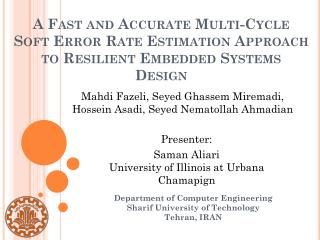
RESULTS (samples) In some results we need more power so we should continue the data capturing or combine the categories of data and subgroups. P<0.0001 Five-year disease free survival according to the stage at diagnosis. (Incidence period 2013-2015. Follow-up date: end of 2018)
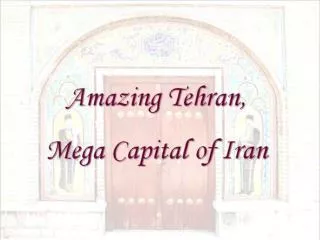
RESULTS (samples) Ongoing analysis of the data captured by the QRN network. In some results we need more power so we should continue the data capturing or combine the categories of data and subgroups. P=0.27 Five-year disease free survival ofthe colon cancer underwent surgery in two teaching centers and one non-teaching. (Incidence period 2013-2015. Follow-up date: end of 2018)
RESULTS About situation of 12 QIs , comparing between centers and benchmarking to the best practices we have received an excellent perspectives of quality of care which will be published soon as a paper.
CONCLUSION • This is the first effort aiming at customizing a model of quality of care assessment for common cancers in Iran. The robustness of the achieved model needs to get evaluated further by policy-makers to become an action model. • “Quality of care registry” is the ultimately desire of utilization of “clinical cancer registry” which we can and we should get it. This is the first steps to approach it.
Final questions • What will be the next steps? • Expanding the network? • Through the similar cancer centers to empower the study • Through the other cancer centers in Iran (medium and small) • Working in more detail and try to have an operational model in real world e.g. the model of authorization for quality of care assessment and try to fix the gap and disparity in this number-limited network, at first?
Sometimes you’ve got to go through the hell to get to heaven. Thank you for your attention.