Download
1 / 32
340 likes | 799 Vues
Esophageal Eosinophilia. Is it due to...? severe GERD Intraepithelial eos correlate w/reflux esophagitis but.. Normal esophageal pH studies Poor response to acid blockade subset of eosinophilic gastroenteritis manifestation of IBD or other autoimmune disorder a new separate disease.

E N D
Esophageal Eosinophilia Is it due to...? • severe GERD • Intraepithelial eos correlate w/reflux esophagitis • but.. • Normal esophageal pH studies • Poor response to acid blockade • subset of eosinophilic gastroenteritis • manifestation of IBD or other autoimmune disorder • a new separate disease
Eosinophilic Esophagitis • Isolated eosinophilic infiltration of esophageal mucosa • Digestive symptoms • Dyspepsia, dysphagia • Can mimic GE reflux • Unresponsive to acid suppression therapy • Emerging disease • Increasing incidence
Chronology • 1953: Schatzki’s ring reported • Possible association with EE • 1970s: “Felinized” esophagus reported • Multiple concentric rings attributed to GERD or congenital anomaly • 1978: First report of “eosinophilic esophagitis” as separate entity • Landres et al, Gastroenterology 74:1298. • 1982: Correlation established between eos and reflux esophagitis • 1995: Kelly and Sampson demonstrate link between persistent EE and dietary antigens • Improvement with an elemental formula; Gastroenterology 109:1503-12. • 1998: First reports of successful treatment of EE with oral or topical corticosteroids • 2003: First study of natural history of EE in adults published • 2006: First randomized controlled trial of pharmacologic therapy in EE (swallowed fluticasone) published • 2006: First Int’l. Gastrointestinal Eosinophil Research Symposium (FIGERS) begins developing guidelines for diagnosis and management of EE in children
Epidemiology • PREVALENCE • 1.5-3/10000 adults • 4.3/10000 children • Incidence rising • Approaching that of IBD • Family history • 6.8% of patients • Male predilection Noel R et al. N Engl J Med. 2004: 351:940-41.
Clinical Features of EE CHILD Vomiting Heartburn ADOLESCENT Heartburn Dysphagia ADULT Dysphagia Stricture Yan B, Shaffer EA. World J Gastroenterol. 2006
N = 381 Age 9 +/- 3 y 2 cases in 1994, vs. 72 cases reported in 2003 66% male 85% GER sx 18% dysphagia Endoscopy Normal in 32% Despite clearly abnormal histology N = 103 Only 3% identified prior to 2000 Atopic history Rhinoconj. 57% Food allergy sx 46% Wheezing 37% Fam hx atopy 74% Age-dependent clinical features Pediatric Series Liacouras CA et al. Clin Gastroenterol Hepatol. 2005; 3:1198. Noel R et al. N Engl J Med. 2004; 351:940-41.
Clinical Features of Pediatric EE Noel R et al. N Engl J Med. 2004: 351:940-41. Represents median age of presentation
Diagnosis of EE • Requires endoscopy and histology • Strictly defined as dense eosinophilia confined to the esophagus • Eosinophilia also in stomach, small bowel, colon may be due to another EGID, IBD, parasitic or fungal infection, connective tissue disease, neoplasm • Adjunctive modalities • Contrast UGI series: eval. dysphagia • Esophageal pH-metry: exclude acid GER • CBC/d: periph. eosinophil count • Serum IgE level • Future: biomarkers
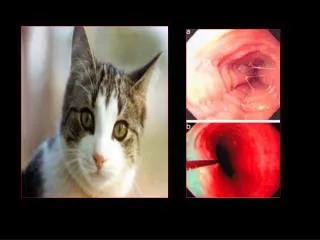
Endoscopy Normal esophagus EE Linear furrowing
Eosinophilic microabscesses Normal “Crepe paper” esophagus Furuta GT, Straumann A. Aliment Pharmacol Ther. 2006;24:173-82.
EE Trachealization Contrast UGI series Fox VL et al, Gastrointestinal Endosc. 2002
EGD: Mucosal pallor UGI: Stricture EUS: Submucosal thickening Fox VL et al, Gastrointestinal Endosc. 2002
Histology • Eosinophils in the esophagus are never normal • Eosinophil count (eos/hpf) alone is not enough to establish dx of EE • >15 eos/hpf suggests EE in the proper clinical context • Pathology report should quantify eos in the most dense field • Multiple biopsies should be taken from distal and proximal sites in esophagus • GERD esophagitis is typically localized to distal esophagus • Inflammation may have “patchy” distribution Ruchelli E, Antonioli D, FIGERS/NASPGHAN Annual Meeting 2006.
Proposed Biomarkers • Non-invasive • Reproducible and predictive • Based on pathophysiology • Sputum eosinophils • Serum CD23 levels • Plasma eotaxin-3 and eosinophil-derived neurotoxin (EDN) levels • Correlated strongly, along with peripheral eosinophil count, with mean esophageal eosinophil density* • mRNA or gene microarray for eotaxins and cytokines (IL-5, IL-13, RANTES) Gupta SK. FIGERS 2006. *Konikoff MR et al. Clin Gastroenterol Hepatol. 2006; 4:1328-36.
Pathogenesis Present understanding: “An immune disorder that results from a mixed allergic response” to dietary and possibly other environmental antigens* Th-2 response IL-5 key for eosinophil differentiation, activation Eotaxins, IL-4, IL-13 recruit eos to GI tract Chronic allergy Kay AB. New Engl J Med. 2001 *Markowitz JE, Liacouras CA. Dig Liver Dis. 2006; 38:251-53.
Pathogenesis • Once in GI tract, eos release eotaxins, IL-5, GM-CSF, PAF and attract more eos • Eos cause local inflammation by releasing MBP, cytotoxic granule contents, more cytokines • Ongoing inflammation can lead to fibrosis, stenosis, morphologic alteration Rothenberg ME. New Engl J Med. 1998
Role of Environmental Allergens • Seasonal exacerbation in some cases • Association with pollen allergy • Atopic background of many EE patients • Experimental EE (mouse models) • Respiratory allergens induced EE while oral or intragastric ones did not • Intratracheal IL-13 induced EE • Deficiency in IL-5, eotaxin-3 and its receptor, and STAT-6 protected mice vs. EE Mishra A et al. J Clin Invest. 2001; 107:83-90. Rothenberg ME. FIGERS and NASPGHAN Annual Meeting 2006.
Blanchard C et al. J Allergy Clin Immunol. 2006; 118: 1054-9.
Natural History • In general, the disease “stays around” • No mortality but persistent morbidity • No evidence of dysplasia or malignant transformation • Complications of untreated EE • Esophageal stricture • Food impaction • Sliding hiatal hernia (esoph. shortening) • Tracheal edema • Subglottic stenosis • Superinfection with Candida or CMV • Risk of emesis-induced or endoscopic perforation
Natural History • Based on limited data • 30 adult patients followed for up to 11 years* • No adverse impact on nutritional status • No worsening of sx, but no histologic improvement • 24 pediatric patients who refused tx or were lost to follow-up** • Mean follow-up 6 yrs later • All had persistent eosinophilia • 20 who had presented with GER sx came back with dysphagia • N=89 (CCH 8 yr retrospective): of 66% of the patients who had initial resolution, 79% later relapsed*** • Chronic disease at best, progressive at worst • Progression: esophagitisringssmall caliberpermanent fibrosis and stricture • Histologic relapse off therapy is common • Absence of sx does not predict absence of inflammation • Effectively treated patients have not been observed to develop dysphagia or fibrosis * Straumann A et al. Gastroenterology 2003. ** Liacouras CA, Putnam P. FIGERS 2006. ***Assa’d A et al. J Allergy Clin Immunol. 2007.
31 children with EE • Fluticasone 880 mcg/d PO X 3 months • Induced remission (lowered peak eos ct to <1) • Improved endoscopic and histologic features • Reduced vomiting • Reduced esoph. CD8+ T cells and mast cells • Was safe • Responders • Non-allergic (neg. SPT) • Younger, shorter, lighter
Kelly & Sampson, 1995 N = 10 children Strict AA formula X 6 w 100% clin/histol response 80% remission Markowitz et al., 2003 N = 51 children, 48/51 responded to AA-based formula (Neocate 1+) NG tube in all but 3 Liacouras et al., 2006 N = 381 over 10 years 172 tx’d with AA-based formula 128 required NGT Eos/hpf Pre-diet: 38.7 Post: 1.1 75 tx’d with elimination diet based on SPT/APT Spergel et al., 2005 Elim. Diet based on SPT/APT Kagalwalla et al., 2006 Six food elimination diet CMP, soy, egg, wheat, peanut, seafood Dietary Therapy
Dietary Therapy Six Food Elim. Kagalwalla N = 35 SPT/APT- Directed Spergel N = 146 Elemental Liacouras N = 160 Kagalwalla A et al. Clin Gastroenterol Hepatol. 2006; 4:1077-1102. Spergel JM et al. Ann Allergy Asthma Immunol. 2005; 95:336-43. Liacouras CA et al. Clin. Gastroenterol. Hepatol. 2006; 3:1198.
Combination testing Can identify correct elimination diet in 70% Resolution of sx/bx Specific foods were definitely identified as the cause of EE in 39/146 On elimination bx normalized Reintroduction of the causative foods relapse of symptoms Bx: return of eosinophilic inflammation The combination of the 2 testing methods had an excellent NPV (88% to 100%) for all foods except milk, which was very low at 41% Role of SPT/APT Spergel JM et al., 2007
Khan S, Henderson N (2002) Current Treatment Options in Gastroenterologyg
Do children with EE grow up to be adults with EE? • What is the role in EE pathogenesis of... • food and aeroallergen cross-reactivity? • IgE? • Is there a genetic or phenotypic difference between atopic and non-atopic EE? • What is the prevalence of EE among highly atopic pts? • What is the value of RAST, skin prick testing, and atopic patch testing in dx of EE? • Therapeutic prospective comparisons: • Elemental diet vs. elimination diet vs. corticosteroids • Should endpoint of treatment be... • clinical remission, OR... • normalization of histology?
Paul Ehrlich 1854-1915 Eos GREEK GODDESS OF DAWN