Download
1 / 22
240 likes | 460 Vues
Hypothyroidism in pregnancy. Mary Lacy. Case at the VA. 29yo G2P1 w/ h/o poorly controlled primary hypothyroidism. b-hcg positive on 3/15 and TSH that same day of 101.5. Pt has been on 112mcg of levothyroxine since December when her dose was increased from 88mcg 2/2 TSH of 40.

E N D
Hypothyroidism in pregnancy Mary Lacy
Case at the VA • 29yo G2P1 w/ h/o poorly controlled primary hypothyroidism. b-hcg positive on 3/15 and TSH that same day of 101.5. • Pt has been on 112mcg of levothyroxine since December when her dose was increased from 88mcg 2/2 TSH of 40. • What did we do? • Increased dose to 150mcg based on 1.6mcg/kg and adding 30% for increased demands in pregnancy • Repeat labs (recommended q4-6 weeks in pregnancy rather than q6-8weeks) • Most recent labs (at 11 weeks): • TSH: 39.81 • Free T4: 1.31
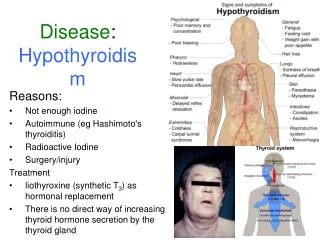
Classifications of Hypothyroidism • Overt Hypothyroidism: 0.3-0.5% of screened women • Increased TSH, Decreased Free T4 • Subclinical Hypothyroidism: 2-2.5% of screened women • Increased TSH, Normal Free T4
Changes in labs during pregnancy • Increased TBG Increased Total T4/Total T3 • secondary to increased Estrogen • Serum TSH decreases early in gestation with rise in free T3/free T4 • Secondary to hCG stimulation of thyroid • normalizes by end of first Trimester • Normal TSH in pregnancy • First trimester: 0.1-2.5 mIU/L • Second Trimester: 0.2-3.0 mIU/L • Third Trimester: 0.3-3.0 mIU/L
Thyroid in Fetal development • Thyroid hormone receptor expressed in fetus at 8-10weeks • Reports of when fetus begins to produce thyroid hormone vary, most reports stated 18 weeks, some said 11-12 weeks
Observational study between 1987 – 1999 in Argentina • Followed 150 consecutive pregnancies of 114 women with primary hypothyroidism (primarily chronic lymphocytic) • 99 women were euthyroid on LT4 • 51 were hypothyroid – 16 with OH, 35 with SCH
TSH < 4 92.6% 0% p<0.006 p<0.006 TSH > 4 66.7% 20.8%
4,657 women screened with TSH/TPO-Ab within first 11 weeks of gestation in Southern Italy • Subset of women with TPO-Ab negativity: • Group A: TSH < 2.5 • Group B: TSH between 2.5 – 5.0 • Study assessed pregnancy loss, pre-term and very pre-term delivery
Retrospective analysis of TSH/freeT4/TPO-Ab in 2nd trimester serum samples of 25,216 pregnant women from 1987-1990 in Maine • 47 women with TSH > 99.7% of all values • 15 women with TSH in 98-99.7% + T4 < 7.75mcg/dL (4.6-12) • Prospective study of 62 children born to mothers with hypothyroidism compared to 124 control children from same schools • 7-9 year old children who were euthyroid at birth underwent 15 test of intelligence, school performance, visual-motor performance, etc.
Prospective study in the Netherlands between January - November 1994 • 448 pregnant women initially assessed • Maternal fT4, TSH, TPO-Ab measured at 12 weeks gestation, 32 weeks gestation, and post-partum • 220 children from uncomplicated pregnancies/deliveries • Neurodevelopment assessed at 10 months
Lowest 5% fT4 • Mean difference in Lowest 5% of free T4 = 14.1* (5.9 – 22.3) • Mean difference in lowest 10% = 7.4* (1.1 – 13.9) • Difference of 10 points on PDI score thought to reflect delay of one month Lowest 10% fT4 Lowest 15% fT4 R = 0.46; p=0.03 Lowest 20% fT4
Observational case-control study in Maine in 2004 – 2006 • Free T4 measured in 5,734 women with normal TSH (0.1-3.5) • Women with free T4 ≤ 3% matched with women in 10-90th % • Measurement of Infant Development (VSID III) at age 2 years
So what should I do? • If Hypothyroidism known prior to pregnancy – target TSH <2.5 (poor) • Thyroxine requirements increase 30-50% by 4-6 weeks (good) • can have patients increase dosing to 9 doses/week • Targeted case finding for hypothyroidism as opposed to universal screening (fair) • Treat overt hypothyroidism (good) • Treat subclinical hypothyroidism • improves obstetrical outcomes (fair) • improves offspring development (poor) • Patients with evidence of thyroid autoimmunity are at risk for OH, monitor them throughout pregnancy (fair)