Download
1 / 1
10 likes | 206 Vues
Chicago Latino Youth in Poverty: The underserved population in receiving mental health services Ivan Irie, MS The Chicago School of Professional Psychology – Chicago, IL. Crisis and Referral Entry Service (CARES). Other Mental Health Services.

E N D
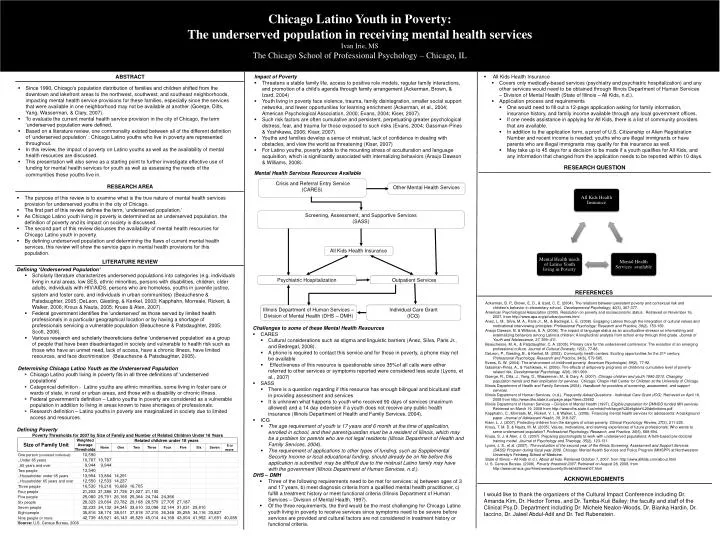
Chicago Latino Youth in Poverty: The underserved population in receiving mental health services Ivan Irie, MS The Chicago School of Professional Psychology – Chicago, IL Crisis and Referral Entry Service (CARES) Other Mental Health Services Screening, Assessment, and Supportive Services (SASS) Psychiatric Hospitalization Outpatient Services Illinois Department of Human Services – Division of Mental Health (DHS – DMH) Individual Care Grant (ICG) ABSTRACT • Impact of Poverty • Threatens a stable family life, access to positive role models, regular family interactions, and promotion of a child’s agenda through family arrangement (Ackerman, Brown, & Izard, 2004) • Youth living in poverty face violence, trauma, family disintegration, smaller social support networks, and fewer opportunities for learning enrichment (Ackerman, et al., 2004; American Psychological Association, 2000; Evans, 2004; Kiser, 2007). • Such risk factors are often cumulative and persistent, perpetuating greater psychological distress, fear, and trauma for those exposed to such risks (Evans, 2004; Gassman-Pines & Yoshikawa, 2006; Kiser, 2007). • Youths and families develop a sense of mistrust, lack of confidence in dealing with obstacles, and view the world as threatening (Kiser, 2007) • For Latino youths, poverty adds to the mounting stress of acculturation and language acquisition, which is significantly associated with internalizing behaviors (Araujo Dawson & Williams, 2008). • Mental Health Services Resources Available • All Kids Health Insurance • Covers only medically-based services (psychiatry and psychiatric hospitalization) and any other services would need to be obtained through Illinois Department of Human Services – Division of Mental Health (State of Illinois – All Kids, n.d.). • Application process and requirements • One would need to fill out a 12-page application asking for family information, insurance history, and family income available through any local government offices. • If one needs assistance in applying for All Kids, there is a list of community providers that are available. • In addition to the application form, a proof of U.S. Citizenship or Alien Registration Number and recent income is needed; youths who are illegal immigrants or have parents who are illegal immigrants may qualify for this insurance as well. • May take up to 45 days for a decision to be made if a youth qualifies for All Kids, and any information that changed from the application needs to be reported within 10 days. • Since 1990, Chicago’s population distribution of families and children shifted from the downtown and lakefront areas to the northwest, southwest, and southeast neighborhoods, impacting mental health service provisions for these families, especially since the services that were available in one neighborhood may not be available at another (Goerge, Dilts, Yang, Wasserman, & Clary, 2007). • To evaluate the current mental health service provision in the city of Chicago, the term ‘underserved population were defined. • Based on a literature review, one commonality existed between all of the different definition of ‘underserved population’ : Chicago Latino youths who live in poverty are represented throughout. • In this review, the impact of poverty on Latino youths as well as the availability of mental health resources are discussed. • This presentation will also serve as a starting point to further investigate effective use of funding for mental health services for youth as well as assessing the needs of the communities these youths live in. RESEARCH QUESTION RESEARCH AREA • The purpose of this review is to examine what is the true nature of mental health services provision for underserved youths in the city of Chicago. • The first part of this review defines the term, ‘underserved population.’ • As Chicago Latino youth living in poverty is determined as an underserved population, the definition of poverty and its impact on society is discussed. • The second part of this review discusses the availability of mental health resources for Chicago Latino youth in poverty. • By defining underserved population and determining the flaws of current mental health services, this review will show the service gaps in mental health provisions for this population. All Kids Health Insurance LITERATURE REVIEW • Defining ‘Underserved Population’ • Scholarly literature characterizes underserved populations into categories (e.g. individuals living in rural areas, low SES, ethnic minorities, persons with disabilities, children, older adults, individuals with HIV/AIDS, persons who are homeless, youths in juvenile justice, system and foster care, and individuals in urban communities)(Beauchesne & Patsdaughter, 2005; DeLeon, Giesting, & Kenkel, 2003; Kapphahn, Morreale, Rickert, & Walker, 2006; Krous & Nauta, 2005; Kruse & Aten, 2007). • Federal government identifies the ‘underserved’ as those served by limited health professionals in a particular geographical location or by having a shortage of professionals servicing a vulnerable population (Beauchesne & Patsdaughter, 2005; Scott, 2006). • Various research and scholarly theoreticians define ‘underserved population’ as a group of people that have been disadvantaged in society and vulnerable to health risk such as those who have an unmet need, lack of access, have a chronic illness, have limited resources, and face discrimination (Beauchesne & Patsdaughter, 2005). • Determining Chicago Latino Youth as the Underserved Population • Chicago Latino youth living in poverty fits in all three definitions of ‘underserved populations’ • Categorical definition - Latino youths are ethnic minorities, some living in foster care or wards of state, in rural or urban areas, and those with a disability or chronic illness. • Federal government’s definition – Latino youths in poverty are considered as a vulnerable population in addition to living in areas known to have shortages of professionals. • Research definition – Latino youths in poverty are marginalized in society due to limited access and resources. • Defining Poverty REFERENCES Ackerman, B. P., Brown, E. D., & Izard, C. E. (2004). The relations between persistent poverty and contextual risk and children's behavior in elementary school. Developmental Psychology, 40(3), 367-377. American Psychological Association (2000). Resolution on poverty and socioeconomic status. Retrieved on November 16, 2007, from http://www.apa.org/pi/urban/povres.html Anez, L. M., Silva, M. A., Paris Jr., M., & Bedregal, L. E. (2008). Engaging Latinos through the integration of cultural values and motivational interviewing principles. Professional Psychology: Research and Practice, 39(2), 153-159. Araujo Dawson, B. & Williams, S. A. (2008). The impact of language status as an acculturative stressor on internalizing and externalizing behaviors among Latino/a children: A longitudinal analysis from school entry through third grade. Journal of Youth and Adolescence, 37, 399–411. Beauchesne, M. A., & Patsdaughter, C. A. (2005). Primary care for the underserved conference: The evolution of an emerging professional culture. Journal of Cultural Diversity, 12(3), 77-88. DeLeon, P., Giesting, B., & Kenkel, M. (2003). Community health centers: Exciting opportunities for the 21st century. Professional Psychology, Research and Practice, 34(6), 579-585. Evans, G. W. (2004). The environment of childhood poverty. American Psychologist, 59(2), 77-92. Gassman-Pines, A., & Yoshikawa, H. (2006). The effects of antipoverty programs on children's cumulative level of poverty-related risk. Developmental Psychology, 42(6), 981-999. Goerge, R., Dilts, J., Yang, D., Wasserman, M., & Clary, A. (2007). Chicago children and youth 1990-2010: Changing population trends and their implication for services. Chicago: Chapin Hall Center for Children at the University of Chicago. Illinois Department of Health and Family Services (2004). Handbook for providers of screening, assessment, and support services. Illinois Department of Human Services. (n.d.). Frequently Asked Questions - Individual Care Grant (ICG). Retrieved on April 16, 2008 from http://www.dhs.state.il.us/page.aspx?item=33652 Illinois Department of Human Services – Division of Mental Health (1997). Eligible population for DMHDD funded MH services. Retrieved on March 19, 2008 from http://www.dhs.state.il.us/mhdd/mh/target%20eligible%20definitions.pdf Kapphahn, C., Morreale, M., Rickert, V. I., & Walker, L. (2006). Financing mental health services for adolescents: A background paper. Journal of Adolescent Health, 39, 318-327. Kiser, L. J. (2007). Protecting children from the dangers of urban poverty. Clinical Psychology Review, 27(2), 211-225. Krous, T. M. D. & Nauta, M. M. (2005). Values, motivations, and learning experiences of future professionals: Who wants to serve underserved population? Professional Psychology, Research, and Practice, 36(6), 688-694. Kruse, S. J. & Aten, J. D. (2007). Preparing psychologists to work with underserved populations: A faith-based pre-doctoral training model. Journal of Psychology and Theology, 35(2), 123-131. Lyons, J. S., et al. (2007). The evaluation of the second year of the Illinois Screening, Assessment and Support Services (SASS) Program during fiscal year 2006. Chicago: Mental Health Services and Policy Program (MHSPP) at Northwestern University’s Feinberg School of Medicine. State of Illinois – All Kids (n.d.). About all kids. Retrieved October 7, 2007, from http://www.allkids.com/about.html U. S. Census Bureau. (2008). Poverty threshold 2007. Retrieved on August 28, 2008, from http://www.census.gov/hhes/www/poverty/threshld/thresh07.html • Challenges to some of these Mental Health Resources • CARES • Cultural considerations such as stigma and linguistic barriers (Anez, Silva, Paris Jr., and Bedregal, 2008). • A phone is required to contact this service and for those in poverty, a phone may not be available • Effectiveness of this resource is questionable since 35%of all calls were either referred to other services or symptoms reported were considered less acute (Lyons, et al., 2007) • SASS • There is a question regarding if this resource has enough bilingual and bicultural staff in providing assessment and services • It is unknown what happens to youth who received 90 days of services (maximum allowed) and a 14 day extension if a youth does not receive any public health insurance (Illinois Department of Health and Family Services, 2004). • ICG • The age requirement of youth is 17 years and 6 month at the time of application, enrolled in school, and their parent/guardian must be a resident of Illinois, which may be a problem for parents who are not legal residents (Illinois Department of Health and Family Services, 2004). • The requirement of applications to other types of funding, such as Supplemental Security Income or local educational funding, should already be on file before this application is submitted may be difficult due to the mistrust Latino family may have with the government (Illinois Department of Human Services, n.d.). • DHS – DMH • Three of the following requirements need to be met for services: a) between ages of 3 and 17 years, b) meet diagnosis criteria from a qualified mental health practitioner, c) fulfill a treatment history or meet functional criteria (Illinois Department of Human Services – Division of Mental Health, 1997). • Of the three requirements, the third would be the most challenging for Chicago Latino youth living in poverty to receive services since symptoms need to be severe before services are provided and cultural factors are not considered in treatment history or functional criteria. ACKNOWLEDGMENTS I would like to thank the organizers of the Cultural Impact Conference including Dr. Amanda Kim, Dr. Hector Torres, and Dr. Tamba-Kuii Bailey; the faculty and staff of the Clinical Psy.D. Department including Dr. Michele Nealon-Woods, Dr. Bianka Hardin, Dr. Iaccino, Dr. Jaleel Abdul-Adil and Dr. Ted Rubenstein.