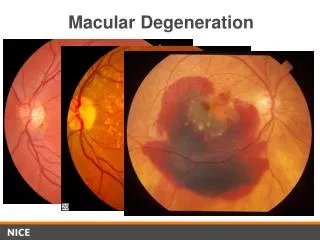
Acquired Macular Disorders
Acquired Macular Disorders. April 01, 2008. Idiopathic Central Serous Chorioretinopathy (ICSC). Transient episodes of serous retinal or RPE detachments in the macula. No predisposing retinal signs Drusen. ICSC: Characteristics. Male, caucasian, 25 to 45 years old Unilateral

Acquired Macular Disorders
E N D
Presentation Transcript
Acquired Macular Disorders April 01, 2008
Idiopathic Central Serous Chorioretinopathy (ICSC) • Transient episodes of serous retinal or RPE detachments in the macula. • No predisposing retinal signs • Drusen
ICSC:Characteristics • Male, caucasian, 25 to 45 years old • Unilateral • Type A personality • Vascular excitability creating a localized breakdown in choriocapillaris blood supply to the RPE.
ICSC:Clinical Appearance • BIO: • Dome of elevated retina • Look for color variations, reflections off the ILM, loss of FLR • Fundus lens: • Retinal vessels within the CSR area will cast shadows onto the attached RPE. • Yellow precipitates – poorer prognosis.
Chronic ICSC:Precipitates “Lemon-drop nodules”
ICSC:Clinical Findings • Fairly sudden visual acuity reduction. • 20/40 • A hyperopic refractive shift. • Relative scotoma, metamorphopsia, micropsia, and impaired dark adaptation.
ICSC: • About 80% of ICSC cases spontaneously resolve in 6 months. • Mild metamorphopsia can remain. • Permanent visual acuity reduction or disturbance. • prolonged detachment or recurrent attacks • 20% recurrent rate • Focal laser if VA decrease is significant.
ICSC:Other Diagnostic Testing • Fluorescein angiography • typically shows a 'smokestack' and 'umbrella' or 'mushroom' hyperfluorescence (late venous phase) • OCT
ICSC: OCT
CME • Accumulation of fluid within the macula. • Layers affected typically are the outer plexiform (Henle's fiber) layer and the inner nuclear layer. • Macular thickening occurs with multiple cystic areas.
CME:Causes • Post-op cataract (Irvine –Gass syndrome) • Post YAG capsulotomy • Retinal surgery • Intraocular inflammation • Retinal vascular conditions
CME: Clinical Appearance • Often seen as just a loss of the FLR • Prolonged photostress recovery test • Any other clinical tests?
CME:Fluoroscein angiography • Petalliform appearance
CME: OCT
CME:Management • Depends on underlying cause: • Laser photocoagulation vascular cases (i.e. retinal vein or arterial occlusions • Steroids and non-steroidal anti-inflammatory drugs (Triamcinolone)
ERM: • AKA - premacular gliosis, cellophane maculopathy, surface-wrinkling retinopathy, preretinal fibrosis, and macular pucker • Occur as the result of proliferation of retinal glial cells on the ILM that have escaped through breaks in the ILM.
ERM:Treatment • Vitrectomy and membrane peeling • indicated only if significantly reduced visual acuities.
ERM: Vitrectomy and membrane peeling
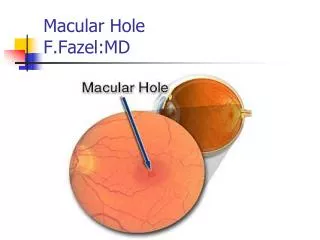
Macular holes: • Results from a perifoveal focal vitreous cortex contraction. • pulls the macular tissue free from the choroid. • typically spontaneous and abrupt • bilateral in only 10 percent of cases.
Etiologies of macular hole: • Idiopathic (affects mainly postmenopausal women) • Severe Myopia (associated with posterior staphylomas) • Trauma (vitreous traction or commotio retinae) • Solar Retinopathy (very small lamellar hole or cyst, 2 weeks post-UV exposure
Stages of macular holes: Stage 1: Decreased or absent foveal depression. Small round yellow spot/ring in fovea. Macular cyst Stage 2: Tangental tear at one edge of fovea.
Stages of macular holes: Stage 3: Round punched-out area about 1/3 disc diameter. Halo of retinal detachment surround. Visual acuity usually 20/200 or worse. Stage 4: Complete hole Edematous ‘cuff’ at margins
Macular hole stages: 1 2 3 4
Treatment of Macular holes Treatment of macular holes involve ILM peeling and vitrectomy. • relieves vitreo-retinal traction • stimulates glial cell proliferation and migration into the macular area
Toxic maculopathies • Exogenous substances causing potential toxicity to the macula. • Antimalarials • Phenothiazines • Tamoxifen • Talc
Plaquenil (Hydroxychloroquine): • Used to treat malaria and rheumatological disorders (i.e. rheumatoid arthritis, lupus). • Tends to concentrate in melanin-containing structures such as the RPE and choroid • Excess of 300g cumulative oral dose (250mg/day for 3 years) significantly increases risk of maculopathy.
Plaquenil Maculopathy: • Classically presents as "bullseye" maculopathy. • A pre-treatment baseline retinal evaluation: • Visual acuities • Amsler grid • Color vision • Visual fields (10-2, Macular Threshold) • Dilated retinal examination • Fundus photos • Post-treatment evaluations repeated every 6 to 12 months.
Plaquenil Maculopathy: • VA ranges: • 20/30 to 20/40 BCVA • faint halo of RPE pallor • 20/60 to 20/80 BCVA • dark ring surrounds halo (Bull’s eye macula) • VF changes: • Scotoma to red target between 4-9 degrees.
Plaquenil maculopathy: • 10-2 HVF • Red Target
Phenothiazine: • Thioridazine (Melleril) • normal dose is 150 to 600mg/day • greater than 800mg/day for a few weeks can cause retinotoxicity • Chlorpromazine (Largactil) • normal is 75 to 300mg/day • greater than 2400mg/day over many weeks can cause retinotoxicity
Phenothiazine Maculopathy: • Retinopathy presents as a “salt and pepper” appearance to the macula. • A coarse granular macular pigmentation • usually appears first • Decreased visual acuities and poor dark adaptation. • May not progress if drug is discontinued. • Geographic RPE/choriocapillaris atrophy with hyperpigmented clumps with continued drug use.
Tamoxifen: • (Nolvadex, Emblon, Noltam, Tamofen) • is an anti-estrogen used to treat breast carcinoma. • normal dose of 20 to 40mg/day • current dosages prescribed today are usually less.
Tamoxifen Maculopathy: • Presents as multiple superficial yellow crystalline ring-like deposits at the macula. • can cause visual acuity loss • Also – A vortex keratopathy and optic neuritis can rarely occur.