Download
1 / 35
360 likes | 600 Vues
Quality Initiatives: Physician Leadership in the Emergency Department . On the CUSP: Stopping CAUTI at the Front Door NJHA – August 15, 2013. David J. Adinaro MD, MAEd , FACEP President, NJ-ACEP Chief , Adult Emergency Department, SJRMC EM Residency Research Director, SJRMC.

E N D
Quality Initiatives: Physician Leadership in the Emergency Department On the CUSP: Stopping CAUTI at the Front Door NJHA – August 15, 2013
David J. Adinaro MD, MAEd, FACEP President, NJ-ACEP Chief, Adult Emergency Department, SJRMC EM Residency Research Director, SJRMC
Disclosures • I have nothing to report in terms of financial disclosures. • My opinions are my • own.
Biases • That I have the best job in the world • That I work with the best people in the best profession • That we do noble work I believe
Biases • That I have the best job in the world • That I work with the best people in the best profession • That we do noble work • That we can do better I believe
Objectives • ED Physicians role in preventing CAUTI • Identify the opportunities to change physician behavior • Importance of collaboration in ED to change systems and cultures
The Sharp End • Where the work is done and errors are made\discovered • Real time decisions based on available information • Last line of defense in error prevention • In healthcare made up of doctors, nurses, techs
The Blunt End • Distal to the sharp (work end) • Often remote from real time decisions but contribute to the care given and errors made • ED Exec, Hospital Administration, State regulations, National Policies
Reason’s Model of Normal Accidents ED physician orders Foley need not reevaluated on floor Lack of institutional policy or goal Family requests Admitting physician does not address Patient develops CAUTI
Preventing CAUTI at the Front Door • ED Physician Role in Preventing CAUTI
Preventing CAUTI at the Front Door • In theory placement of a foley catheter needs a physician order. • Good evidence based indications for placement
Preventing CAUTI at the Front Door • KT (Knowledge Translation) Approach • Lack of knowledge about consequences • Lack of consequence • Prior training • Lack of alternatives • Systems approach • This is how we do it • Changing the easiest pathway
Preventing CAUTI at the Front Door • Great summary article from a respected elder of emergency medicine • http://www.epmonthly.com/columns/in-my-opinion/rick-bukata-the-high-cost-of-convenience-caths/
Preventing CAUTI at the Front Door • Also reviewed the inappropriate indications for catheter placement: • Incontinence (without additional indication) • Diuresis • Frequent, nonessential measurement of UOP • Nurse’s concern about patient discomfort • Diarrhea (without additional indication) • Patient’s preference
Preventing CAUTI at the Front Door • Identify the opportunities to change physician behavior
Preventing CAUTI at the Front Door • “Small Wins” Approach • Academic detailing\Physician Champion • Group responsibility • Monthly or quarterly data • Trend Foleys and infections • Individual responsibility • Audit and feedback • Inclusion in yearly reviews
Preventing CAUTI at the Front Door • Small Wins – produce change without confronting the system directly or aggressively. • Impact is from examples they provide others. • Through doing something tangible. • Through showing change is possible.
Preventing CAUTI at the Front Door • Academic Detailing\Physician Champion • Physician Champion • Unlikely to be chairman\ED director • Tend to have a full plate. • Champions need to have ability to focus on the project for at least a year. • Ayounger (training-wise) doc with some stature in department.
Preventing CAUTI at the Front Door • Group responsibility • Tends to be least threatening to individual physician • Monthly or quarterly data • Trend Foleys and related infections
Preventing CAUTI at the Front Door • Group responsibility • Usually a good first step • Will usually get attention of “center of department” • Ineffectual for outliers
Preventing CAUTI at the Front Door • Individual responsibility • Audit and Feedback • Yearly reviews • Best for outliers
Preventing CAUTI at the Front Door • Audit and Feedback methodology: • Mentioned frequently in KT literature • Fits in with Plan, Do, Study, Act cycles • Really just behavioral reinforcement to effect change • Most basic and probably most effective
Preventing CAUTI at the Front Door • Audit and Feedback methodology: • Based on clearly defined guidelines • Must be on-going and as real-time as possible • Should include a mechanism to address systemic (non individual) issues.
Preventing CAUTI at the Front Door • Audit and Feedback methodology: • Real-time feedback (days\weeks not months) • Feedback from consistent source (physician champion) • Feedback is on success and failure • Include alternatives
Preventing CAUTI at the Front Door • Importance of collaboration in ED to change systems and cultures
ED Collaborations PICTURE
ED Collaborations • Department is made up of physicians and nurses • No one group fixes any problem without the other • Likelihood of success lower without close integration • Unlikely in future medicine will be successful without collaborative leadership and care • Proximity is not enough!
ED Collaborations • SJRMC • Paterson, NJ • 150,000 visits • 50 physicians, 120+ nurses • 2008 – ED Exec Team • 2009 - EDQA Committee
ED Collaboration • ED EXEC • ED Physician and ED Nurse leadership • Formally meets weekly • Informally constantly • Joint decision making • Unified Implementation • Message travels separate pathways
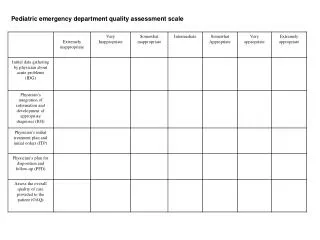
ED Collaboration • EDQA • Off shoot of ED Exec • Open meetings • Open, “anonymized” referral process • Screens used • Separate from Audit and Feedback related to quality initiative (STEMI, pneumonia, stroke)
ED Collaboration • EDQA • Relies on an established worksheet • Examines individual care provided and systems involved • Key in identifying system\cultural strengths and weakness • Forms the basis of many decisions made by ED EXEC
ED Collaboration • EDQA • To date reviewed over 1,000 cases • Majority have no findings\concerns • Feedback provided to treating staff • CME\contact hours available • Highlights excellent care also
Preventing CAUTI at the Front Door • ED Physician Role in Preventing CAUTI • Identify the opportunities to change physician behavior • Importance of collaboration in ED to change systems and cultures
Thank You! • Adinarod@sjhmc.org • @PatersonER • PatersonER.com (blog) • Slides available • NJEmergencyDocs.com (acep blog)