Download
1 / 84
870 likes | 1.23k Vues
Family Paramyxoviridae Subfamily Paramyxovirinae: Genes : Morbillivirus – measles virus, Respirovirus (earlier Paramyxovirus) – parainfluenza virus serotypes 1 and 3 Rubulavirus - parainfluenza virus serotypes 2, 4а, 4 b, mumps virus Subfamily Pneumovirinae

E N D
FamilyParamyxoviridae SubfamilyParamyxovirinae: Genes: Morbillivirus – measles virus, Respirovirus (earlierParamyxovirus) – parainfluenza virusserotypes 1 and 3 Rubulavirus - parainfluenza virusserotypes 2, 4а, 4b, mumps virus Subfamily Pneumovirinae Genes: Pneumovirus – RS-virus Metapneumovirus
Properties of the Paramyxoviruses A.Structure: The particle has a lipid-containing envelope covered with spikes; a helical ribonucleoprotein nucleocapsid 18 nm in diameter is enclosed. The RNA is a single molecule (MW 5-8 x 106).
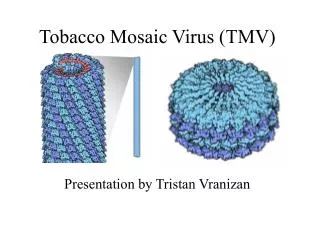
PARAMYXOVIRUSES pleomorphic HN/H/G glycoprotein SPIKES F glycoprotein SPIKES helical nucleocapsid (RNA minus NP protein) lipid bilayer membrane polymerase complex M protein
The envelope of paramyxoviruses contains 2 glycoproteins, HN and F, that form spikelike projections from the surface of the viral membrane. These glycoproteins are involved in the early interactions between virus and cell. The larger glycoprotein, HN, has neuraminidase and hemagglutinating activities and is responsible for virus adsorption. The other glycoprotein, F, is involved in virus-induced cell fusion and hemolysis and in virus penetration through fusion of viral and cell membranes. The membrane-fusing activity of Ihe F protein is activated by proteolytic cleavage of a precursor (Fo) by a host enzyme to yield 2 disulfide-linked polypeptides (F1 and F2). Only then can viral replication begin.
HN: Larger virus glycoprotein, responsible both for hemagglutinatlon and receptor-destroying activities of the virus particle. F: Smaller virus glycoprotein, Involved In cell fusion by these viruses and probably in the entry of the virus Into the cell. F is composed of 2 disulfide bond-linked polypeptides cleaved from a high-molecular-weight precursor. Lipid bilayer: The lipid is cell-derived but probably altered in composition from that of the normal cell. M: Nonglycosylated membrane protein. The HN, F, M, and lipid bilayer can be disrupted, destroying hemolytic activity, and then reassembled without the nucleocapsid, whereupon hemolytic activity is restored. NP: Ribonucleoprotein, the major complement-fixing antigen. There is another small protein of about 47,000 molecular weight whose location and function in the virion are unknown.
B. Biologic Properties: 1. Cell fusion. In the course of infection, paramyxoviruses cause cell fusion, long recognized as giant cell formation. This ability to fuse cells is now used for the creation of cell hybrids, an important tool in somatic cell genetics. 2. Persistent infection. Most paramyxoviruses can produce a persistent noncytocidal infection of cultured cells. The clinical importance of this property may explain subacute sclerosing panencephalitis (SSPE). 3. Antigenic properties. Measles, canine distemper, and rinderpest viruses have related antigens. Another antigenically related group includes mumps, parainfluenza, and Newcastle disease viruses.
C. Replication. The RNA genome of viruses of this group is not infectious and does not function as messenger RNA. Instead, the viral genome is transcribed into shorter RNA molecules that serve as messenger and are complementary to the genome. The paramyxoviruses possess an RNA-dependent RNA polymerase that is a structural component of the virion and produces the initial messenger RNA.
MUMPS (Epidemic Parotitis) Mumps is an acute contagious disease characterized by a nonsuppurative enlargement of one or both of the parotid glands, although other organs may also be involved. Properties of the Virus Mumps virus is a typical paramyxovirus. A. Morphology and Biochemical Properties. The mumps virus particle has the typical paramyxovirus morphology. Typical also are the biologic properties of hemagglutination, neuraminidase, and hemolysin. Hemagglutination can be inhibited by specific antisera to mumps virus, and this inhibition can be used to measure antibody responses. Similarly, the nucleocapsid of the virus particle forms the major component of the "S" (soluble) complement-fixing antigen.
B. Reactions to Physical and Chemical Agents. The hemagglutinin, the hemolysin, and the infectivity of the virus are destroyed by heating at 56 °C for 20 minutes. The skin test antigen and the complement-fixing antigen are more heat-stable. C. Animal Susceptibility and Growth of Virus. In monkeys, mumps can produce a disease that is very much like that in human beings. Parotitis is produced by introducing the virus into Stensen's duct or directly into the gland by injection. By the use of fluorescent antibody, the virus has been located in the cytoplasm of acinar cells. The virus grows readily in embryonated eggs and in cell culture. Passage in embryonated eggs reduces pathogenicity for humans, and this method was used to obtain a vaccine strain. Mumps virus growing in cell culture produces multinucieated giant cells (syncytia).
D. Skin Test. A skin test antigen for determining hypersensitivity to mumps virus is available, A positive test is considered to be erythema and induration greater than 15 mm 24-48 hours after injection. The skin lest is of uncertain value in predicting immune status, since both false positives and false negatives occur frequently.
Pathogenesis and Pathology Two theories exist regarding the pathogenesis of mumps. (1) The virus travels from the mouth by way of Stensen 's duct to the parotid gland, where it undergoes primary multiplication. This is followed by a generalized viremia and localization in testes. ovaries, pancreas, thyroid, or brain. (2) Primary replication occurs in the superficial epithelium of the respiratory tract. This is followed by a generalized viremia and simultaneous localization in the salivary glands and other organs. Little tissue damage is associated with uncomplicated mumps. The ducts of the parotid glands show desquamation of the epithelium, and polymorphonuclear cells are present in the lumens. There are interstitial edema and lymphocytic infiltration. With severe orchitis, the testis is congested, and punctate hemorrhage as well as degeneration of the epithelium of the seminiferous tubules is observed. Central nervous system pathology may vary from perivascular edema to inflammatory reaction, glial reaction, hemorrhage, or demyelination.
Clinical Features The incubation period is commonly 18-21 days. A prodromal period of malaise and anorexia is followed by rapid enlargement of parotid glands as well as other salivary glands. Swelling may be confined to one parotid gland, or one gland may enlarge several days before the other. The gland enlargement is associated with pain, especially when tasting acid substances- The salivary adenitis is commonly accompanied by low-grade fever and lasts for approximately a week. The testes and ovaries may be affected, especially after puberty. Twenty percent of males over 13 years of age who are infected with mumps virus develop orchitis, which is often unilateral and does not usually lead to sterility. Because of the lack of elasticity of the tunica albuginea, which does not allow the inflamed testis to swell, atrophy of the testis may follow secondary to pressure necrosis. Secondary sterility does not occur in women because the ovary, which has no such limiting membrane, can swell when inflamed.
Mumps accounts for 10-15% of aseptic meningitis observed in the USA and is more common among males than females. Meningoencephalitis usually occurs 5-7 days after the inflammation of the salivary glands, but it may occur simultaneously or in the absence of parotitis and is usually self-limiting. The cerebrospinal fluid shows pleocytosis (10-2000//n,L, mostly lymphocytes) that may persist after clinical recovery. Rare complications of mumps include (1) a self-limiting polyarthritis that resolves without residual deformity; (2) pancreatitis associated with Transient hyperglycemia, glycosuria, and steatorrhea (it has been suggested that diabetes mellitus may occasionally follow); (3) nephritis; (4) thyroiditis; and (5) unilateral nerve deafness (hearing loss is complete and permanent) . Mumps may be a possible causative agent in the production of aqueductal stenosis and hydrocephalus in children. Injection of mumps virus into suckling hamsters has produced similar lesions.
Laboratory Diagnosis Laboratory studies are not usually required to establish the diagnosis of typical cases. However, mumps can sometimes be confused with enlargement of the parotids due to suppuration, foreign bodies in the salivary ducts, tumors, etc. In cases without parotitis, particularly in aseptic meningitis, the laboratory can be helpful in establishing the diagnosis. A. Recovery of Virus: Virus can be isolated from saliva, cerebrospinal fluid, or urine collected within 4 days after onset of illness. After treatment with antibiotics, the specimens are inoculated into monkey kidney cell cultures. Virus growth can be detected in 5-6 days by adsorption of suitable erythrocytes by the infected cells. The isolate can be identified with specific antiserum that can inhibit the hemadsorption. Immunofluorescent serum can also identify a virus isolate in cell culture within 2-3 days.
B. Serology. Antibody rise can be detected in paired sera. The CF test is best for specificity and accuracy, although the HI test may be used. A 4-fold or greater rise in antibody titer is evidence of mumps infection. A CF test on a single serum sample obtained soon after onset of illness may serve for a presumptive diagnosis. S (soluble) antibodies develop within a few days after onset and sometimes reach a high titer before V (viral) antibodies can be detected. In early convalescence, both S and V antibodies are present at high levels. Subsequently, S antibodies disappear more rapidly, leaving V antibodies as a marker of previous infection for several years. The intradermal injection of inactivated virus results in reappearance of V antibodies in high titer. Neutralizing antibodies also appear during convalescence and can be determined in cell culture.
C. Skin Test Antigen: Delayed type hypersensitivity may be noted about 3-4 weeks after onset. The skin test is less reliable than serologic tests to establish evidence of past infection. Immunity Immunity is permanent after a single infection. Only one antigenic type exists. Passive immunity is transferred from mother to offspring; thus it is rare to see mumps in infants under age 6 months. Treatment Gamma globulin is of no value for decreasing the incidence of orchitis, even when given immediately after parotitis is first noted.
Epidemiology Mumps occurs throughout the world endemically throughout the year. Outbreaks occur where crowding favors dissemination of the virus. The disease reaches its highest incidence in children age 5-15 years, but epidemics occur in army camps. Although morbidity rates are high, the mortality rate is negligible, even when the nervous system is involved. Humans are the only known reservoir of virus. The virus is transmitted by direct contact, airborne droplets, or fomites contaminated with saliva and, perhaps, urine. The period of communicability is from about 4 days before to about a week after the onset of symptoms. More intimate contact is necessary for the transmission of mumps than for measles or varicella.
About 30-40% of infections with mumps virus are inapparent. Individuals with subclinical mumps acquire immunity. During the course of inapparent infection, they can serve as sources of infection for others. Antibodies to mumps virus are transferred across the placenta and are gradually lost during the first year of life. In urban areas, antibodies are then acquired gradually, so that the 15-year-old group has about the same prevalence of persons with antibodies as the adult group. Antibodies are acquired at the same rate by persons living under favorable and unfavorable socio-economic conditions.
Control Mumps is usually a mild childhood disease. A live attenuated vaccine made in chick embryo cell culture is available. It produces a subclinical noncommunicable infection. The vaccine is recommended for children over age 1 year and for adolescents and adults who have not had mumps parotitis, A single dose of the vaccine given subcutaneously produces detectable antibodies in 95% of vaccinees, and antibody persists for at least 8 years. Combination live virus vaccines (measles-mumps-rubella) produce antibodies to each of the viruses in about 95%. In 1967, the year mumps vaccine was licensed, there were about 200,000 mumps cases (and 900 patients with encephalitis) in the USA. After 10 years of vaccine use, the number of mumps cases in 1977 was about 22,000, with 70 cases of encephalitis.
PARAINFLUENZA VIRUS INFECTIONS The parainfluenza viruses are paramyxoviruses with morphologic and biologic properties typical of the genus. They grow welt in primary monkey or human epithelial cell culture but poorly or not at all in the embryonated egg. They produce a minimal cytopathic effect in cell culture but are recognized by the hemad-sorption method. Laboratory diagnosis may be made by the HI, CF, and Nt tests.
PIV- transmission through droplet dispersion(Courtesy-American Assoc. for the Adv. Of Science)
Parainfluenza 1 Included here are Sendai virus, also known as the hemagglutinating virus of Japan (HVJ), and hemadsorption virus type 2 (HA-2). Sendai virus may be a causative agent of pneumonia in pigs and newborn infants. Sendai virus is important in somatic cell genetics, where it is used to produce cell fusion. Clinically, the most important member of this group appears to be the widespread HA-2 virus. It is not cytopathogenic for monkey kidney cell cultures but is detected in such cultures by the hemadsorption test. It is one of the main agents producing croup in children, but it can also cause coryza, pharyngitis, bronchitis, bronchiolitis, or pneumonia. In adults it produces respiratory symptoms like those of the common cold, with reinfection occurring in persons with antibodies from earlier infections. Natural infection stimulates antibody appearance in nasal secretions and concomitant resistance to reinfection, An experimental killed vaccine induces serum antibodies but does not protect against infection
Parainfluenza 2 This group includes the croup-associated (CA) virus of children. The virus grows in human cells (HeLa, lung, amnion) and monkey kidney. Syncytial masses are produced, with loss of cell boundaries. The virus agglutinates chick and human type 0 erythrocytes. Adsorption and hemagglutination occur at 4 °C, and elution of virus takes place rapidly at 37 °C. However, the cells reagglutinate when returned to 4 °C. Mumps patients develop type 2 antibodies. Parainfluenza virus 2 occurs spontaneously in 30% of lots of monkey kidney cells grown in culture, The monkey virus SV5 is antigenically related.
Parainfluenza 3 The viruses in this group are also known as hemadsorption virus type 1 (HA-1). They are detected in monkey kidney cultures by the hemadsorption technique. Serial passage in culture may lead to cytopathic changes. Multinucleated giant cell plaques are produced under agar in certain human cell lines. The virus has been isolated from children with mild respiratory illnesses, croup, bronchiolitis, or pneumonitis. Strains of type 3 virus have been isolated from nasal secretions of cattle ill with a respiratory syndrome known as "shipping fever. At least 70% of market cattle bled at slaughter have parainfluenza 3 antibodies.
Parainfluenza 4 and 5 These viruses are not known to cause any human illness, although antibodies are widespread. Their growth in cell culture can be recognized by the hemadsorption method. Clinical Features and Control Children in the first year of life with primary infections caused by parainfluenza virus type 1, 2, or 3 may have serious illness ranging from laryngo-tracheitis and croup (particularly type 2) to bronchitis, bronchiolitis, and pneumonitis (particularly type 3).
Virtually all infants have maternal antibodies to parainfluenza viruses in serum, yet such antibodies do not prevent infection or disease. Reinfection of older children and adults also occurs in the presence of antibodies arising from an earlier infection. Such rein-fections usually present as nonfebrile upper respiratory infections ("colds"). The incubation for type 1 is 5-6 days; that for type 3 is 2-3 days. Most children have acquired antibodies to all 3 types before age 10. Killed parainfluenza vaccines induce serum antibodies but no immunity. Live vaccines arc being investigated
Virtually all infants have maternal antibodies to parainfluenza viruses in serum, yet such antibodies do not prevent infection or disease. Reinfection of older children and adults also occurs in the presence of antibodies arising from an earlier infection. Such reinfections usually present as nonfebrile upper respiratory infections ("colds"). The incubation for type 1 is 5-6 days; that for type 3 is 2-3 days. Most children have acquired antibodies to all 3 types before age 10. Killed parainfluenza vaccines induce serum antibodies but no immunity. Live vaccines are being investigated
MEASLES (Rubeola) Measles is an acute, highly infectious disease characterized by a maculopapular rash, fever, and respiratory symptoms. Properties of the Virus A. Morphology and Biologic Properties: Measles virus is a typical paramyxovirus, related to canine distemper and bovine rinderpest. All 3 lack neuraminidase activity. Measles agglutinates monkey erythrocytes at 37 °C but does not elute, and it interacts with a distinct cell receptor. Measles virus also causes hemolysis, and this activity can be separated from that of the hemagglutinin.
B. Animal Susceptibility and Growth of Virus: The experimental disease has been produced in monkeys. They develop fever, catarrh, Koplik's spots, and a discrete papular rash. The virus has been grown in chick embryos; in cell cultures of human, monkey, and dog kidney tissue; and in human continuous cell lines. In cell cultures, multinucleate syncytial giant cells form by fusion of mononucleated ones, and other cells become spindle-shaped in the course of their degeneration. Nuclear changes consist of margination of the chromatin and its replacement centrally with an acidophilic inclusion body. Measles virus is relatively unstable after it is released from cells. During the culture of the virus, the intracellular virus liter is 10 or more times the extracellular liter.
Pathogenesis and Pathology The virus enters the respiratory tract, enters cells, and multiplies there. During the prodrome, the virus is present in the blood, throughout the respiratory tract, and in nasopharyngeal, tracheobronchial, and conjunctival secretions. It persists in the blood and nasopharyngeal secretions for 2 days after the appearance of the rash, Transplacental transmission of the virus can occur. Koplik's spots are vesicles in the mouth formed by focal exudations of serum and endothelial cells, followed by focal necrosis. In the skin the superficial capillaries of the corium are first involved, and it is here that the rash makes its appearance. Generalized lymphoid tissue hyperplasia occurs. Multinucleate giant cells are found in lymph nodes, tonsils, adenoids, spleen, appendix, and skin. In encephalomyelitis, there are petechial hemorrhages, lymphocytic infiltration, and. later, patchy demyelination in the brain and spinal cord.
Measles nucleoprotein antigens have been identified by immunofluorescence within inclusion bodies in nerve cells of the brain in subacute sclerosing panencephalitis (SSPE). The virus has been grown by co-cultivating HeLa cells with brain biopsy material or lymph node material from patients. The presence of latent intracellular measles virus in these specimens suggests a tolerant infection with defective cell-mediated immunity. If measles antibody is added to cells infected with measles virus, the viral antigens on the cell surface are altered. By expressing fewer viral antigens on the surface, cells may avoid being killed by antibody- or cell-mediated cytotoxic reactions, yet may retain viral genetic information. This may lead to persistent infection as found in SSPE patients.
Clinical Findings The incubation period is about 10 days to onset of fever and 14 days to appearance of rash. The prodromal period is characterized by fever, sneezing, coughing, running nose, redness of eyes, Koplik's spots (enanthems of the buccal mucosa), and lymphopenia. The fever and cough persist until the rash appears and then subside within 1-2 days. The rash spreads over the entire body within 2-4 days, becoming brownish in 5-10 days. Symptoms of the disease are most marked when the rash is at its peak but subside rapidly thereafter. In measles, the respiratory tract becomes more susceptible to invasion by bacteria, especially hemolytic streptococci; bronchitis, pneumonia, and otitis may follow in 15% of cases.
Encephalomyelitis occurs in about 1:1000 cases. There appears to be no correlation between the severity of the measles and the appearance of neurologic complications. The cause of measles encephalitis is unknown . It has been suggested that early central nervous system involvement is caused by direct viral invasion of the brain. Later appearance of central nervous system symptoms is associated with demyelination and may be an immunopathologic reaction. Symptoms referable to the brain usually appear a few days after the appearance of the rash, often after it has faded. There is a second bout of fever, with drowsiness or convulsions and pleocytosis of the cerebrospinal fluid. Survivors may show permanent mental disorders (psychosis or personality change) or physical disabilities, particularly seizure disorders. The mortality rate in encephalitis associated with measles is about 10-30%, and many survivors (40%) show sequelae.
Measles virus appears to be responsible for sub-acute scterosing panencephalitis (SSPE), a fatal degenerative brain disorder. The disease manifests itself in children and young adults by progressive mental deterioration, myoclonic jerks, and an abnormal dectroencephalogram with periodic high-voltage complexes. The disease develops a number of years after the initial measles infection. Atypical measles. After the introduction of killed measles virus vaccine in 1965, a new clinical syndrome was observed in children who had a history of receiving the vaccine. The syndrome, called atypical measles, was associated with measles virus infection and was characterized by high fever, pneumonia, and an unusual rash (raised papules, wheals, and tiny hemorrhages in the skin) without Koplik's spots. Killed measles virus vaccine is no longer used. Atypical measles is now seen occasionally in young adults.