WORLD IVM EXPERIENCE
WORLD IVM EXPERIENCE. Milton K. H. Leong, M.D. IVF Centre Hong Kong Sanatorium & Hospital, China. LEARNING OBJECTIVES. At the conclusion of this presentation, participants should be able to: Describe the indications IVM Outline the various IVM approaches undertaken currently.

WORLD IVM EXPERIENCE
E N D
Presentation Transcript
WORLD IVM EXPERIENCE Milton K. H. Leong, M.D. IVF Centre Hong Kong Sanatorium & Hospital, China
LEARNING OBJECTIVES At the conclusion of this presentation, participants should be able to: • Describe the indications IVM • Outline the various IVM approaches undertaken currently. • Evaluate the IVM outcomes with regard to the treatment success rates and the babies born as a result of IVM treatment.
DISCLOSURE Milton K. H. Leong, MD None
Development of IVM • It was first demonstrated in 1935 that the immature oocytes have the ability to resume meiosis spontaneously when removed from the follicle. • Pincus G, Enzmann EV. J. Exp. Med. 62, 665-675 (1935) • Edwards showed that in-vitro matured human oocytes could be fertilized. • Edwards RG, Bavister BD, Steptoe PC. Nature. 221(5181), 632-5 (1969).
the immature human oocytes retrieved during gynecologic surgery in an oocyte donation program resulted in the first IVM pregnancy in 1991. • Cha et al., Fertil Steril 55; 109-13 (1991). • 1994-first IVM pregnancy with a patient’s own oocytes. • Trounson A, Wood C, Kausche A. Fertil Steril 62; 353-62 (1994)
Development of the follicle Stage Follicle size (mm) Primordial 0.03 - 0.04 Primary 0.05 - 0.06 Secondary 0.07 - 0.11 Preantral 0.12 - 0.20 Early antral (*) 0.21 - 0.40 Antral (* +) 0.41 - 16.00 Preovulatory (+) 16.10 - 20.00 + IVF * IVM Gougeon, Hum Reprod 1986;1:81-7
Target patient group • Women with high AFC; • PCOS • PCO with regular cycles • The most significant factor which determines the success of IVM treatment is the AFC of the woman (Tan, 2002. Am. J. Obstet. Gynecol. 186; 684-9)
Patient selection for IVM Suikkari 2007; Best Practice & Res Clin Obstet Gynecol 21; 145-155
promising outcomes are also reported in “regular cycling” women Better prognosis if AF basale count > 7 Suikkari 2007; Best Practice & Res Clin Obstet Gynecol 21; 145-155
Common Indications for IVM • failure after > 6 cycles of ovulation induction • women having IVF with high AFC • repeated poor embryo quality in previous IVF cycles for no obvious reason • repeated poor responders to ovarian stimulation
however • low implantation rates when compared to conventional stimulated cycles. • asynchrony in the cytoplasmic and nuclear maturation of the oocyte • asynchrony in the endometrium • culture conditions
Various approaches to improve implantation rates in IVM • Gonadotropin priming • None • hCG • FSH / FSH+hCG • Metformin • IVF / ICSI Clinical Laboratory • Culture conditions
HCG Priming • Theoretically; • Promote invitro maturation • Improve pregnancy rates
IVM following hCG priming • Cycles of IVM 25 • Age (yrs) 35.4 4.7 • Oocytes retrieved 10.3 5.4 • Maturation rate (%) 84 • Fertilization rate (%) 87 • Cleavage rate (%) 95 • Embryos transferred 2.9 0.6 • Clinical pregnancies - no (%) 10 (40) Chian et al New Engl J Med 1999; 341:1624-6
% of metaphase II *p < 0.05 hours of culture Chian et al Hum Reprod 2000; 165-170
Response to LH in granulosa cells from follicles < 8 mm from ovulatory women (with normal ovaries or PCO compared to anovulatory women with PCO)
Duration between HCG administration and oocyte retrieval • When the durations of 35 hours vs. 38 hours between hCG administration and the oocyte retrieval were compared, the 38 h group yielded significantly higher number of mature oocytes. • In-vitro maturation rate after 24 h in the culture was significantly higher, and the clinical pregnancy rate in the 38 h group was higher compared to the 35 h group in the unstimulated cycles, 40.9% vs. 25%. Son et al. Fertil Steril 88(Suppl. 1), S24-S25 (2007).
Clinical outcome in hCG-primed IVM cycles with (Group 1) and without (Group 2) MII-stage oocytes on the day of retrieval Son WY et al. RBM Online. (2008), in press
Hormonal Priming Regular cyclingPCOS • Beneficial • Wynn 1998 • No difference • Trounson 1998 • Suikkari 2000 • Mikkelsen 2005 • Beneficial • Mikkelsen 2001 • No difference • Lin 2003 • Chian 2000
FSH Priming • Results are conflicting • Potential benefits: • Larger ovarian size • Easier retrieval • Higher E2 levels • More maturational competence May improve endometrium
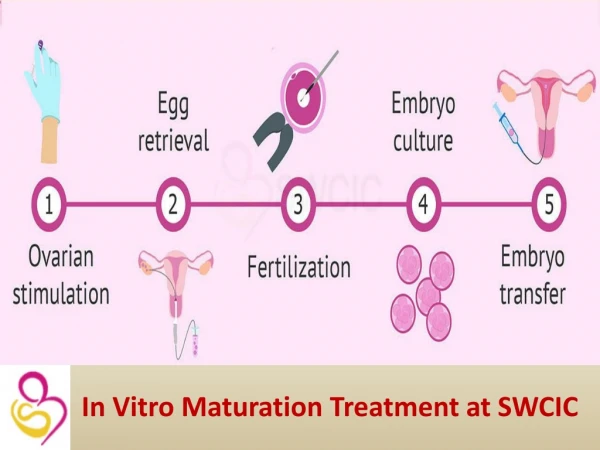
Overview of IVM treatment cycle • Withdrawal bleed • U/S scan day 2-4 to identify if PCO and measure AFC • Repeat u/s scan on day of hCG to measure endometrial thickness • s/c hCG 10,000 IU when ET 6-8 mm, largest follicle 10-12 mm and oocyte retrieval 38 hours later
Transvaginal U/S-guided oocyte retrieval • vaginal vault cleansed with sterile water • i.v. sedation sedation with fentanyl and L.A. • 19 G single single-lumen needle • reduced aspiration pressure (7.5 kPa) • multiple punctures • 10 ml culture tubes with 2ml warm 0.9% saline with 2 IU heparin
In-vitro maturation of oocytes • GV oocytes cultured in IVM medium supplemented with 75mIU/ml FSH + LH for 24 - 48 hrs, checked every 12 hours all MII oocytes undergo ICSI • ET day 2 or 3 following ICSI • Patients receive estradiol-17ß (micronized) immediately following OR and progesteron following ICSI
Endometrial Priming Endometrium is exposed to lower E2 levels Dyssynchrony between phase of endometrium – matured oocyte Endometrial preparation is necessary
Endometrial preparation Endometrial thickness on day of oocyte retrieval <6 mm 10 - 12 mg estradiol-17ß (micronized) 6 - 8 mm 8 - 10 mg estradiol-17ß (micronized) >8 mm 6 mg estradiol-17ß (micronized) Progesterone support (50 mg I/M or 200mg tid, pv) started following ICSI
Can be used in IVM Timing of Oocyte Retrieval Dominant follicle Early atretic follicles Still competent to Embryonic development But; TIMING ?
Timing of Oocyte Collection • Russell et al. (1999) When the leading follicle > 13 mm • Less oocytes • Less fertilization • Fewer embryos
Timing of Oocyte Collection • Cobo et al. (1999) When the leading follicle < 10 mm Higher blastocyst formation
Metformin in IVM • 56 women, 70 cycles • Metformin, 500 mg bid for 12 weeks before the IVM treatment • HMG for 5 days and hCG 10,000 IU, 36 h prior to OPU • number of immature oocytes, oocyte maturation, fertilization and cleavage rates in were comparable to the control group • significantly higher implantation and clinical pregnancy rates were obtained in the metformin-treated group (15.3% and 38.2% respectively) compared to the controls (6.2% and 16.7%) Wei Z et al. Fertil Steril 2007 Nov 15
Outcome of IVM cycles from literature in women with PCO/PCOS.
Outcome of IVM cycles from the literature in women with normal ovaries and regular cycles. * PCO and PCOS groups pooled together.
IVM oocyte donation • 12 oocyte donors (29.7 yrs; AFC 29.7) • oocyte retrieval days 9-18 of unstimulated cycle • mean of 12.8 GV oocytes retrieved • 8.67 mature oocytes and 5.9 fertilized oocytes • 3.9 embryos transferred • implantation rate 19.1%; 6/12 clinical pregnancy – 4 delivered Holzer et al Fertil Steril2007; 88: 62-67
IVM +/- natural cycle IVF and PGD • 35 yr old with RM failed 2 IUI and 2 IVF • IVM offered because of PCO; 1 M II and 14 GV oocytes; ICSI performed • 8 embryos, 6 biopsied, 1 embryo from MII oocyte and 1 from GV oocyte chromosomally normal for 6 autosomes and X and Y chromosome • 2 ET – one blastocyst from MII oocyte and one morula from GV oocyte • ß-hCG 399 IU 14 days after ET and livebirth in May 2005 Ao et al Fertil Steril 2006;85:1510-12
IVM as a Rescue • Some cycles are cancelled due to • Risk of OHSS • Poor pesponse Can IVM be a rescue ? these oocytes can be matured in-vitro
10,000 IU HCG + Immature oocyte retriaval IVM Leading follicle = 12-14 mm IVM as a rescue Risk of OHSS 47 % CLINICAL PREGNANCY No OHSS Lim et al. Fertil Steril 2002
Poor responders no HCG Immature oocyte retrieval + IVM 37,5 % Pregnancy rate Liu et al. Fertil Steril 2003 IVM as a rescue • In POOR RESPONSE = E2 < 1000 pg/ml < 4 mature oocytes
Fertility preservation for young women • Best option; embryo cryopreservation, after ovarian stimulation followed by oocyte retrieval and fertilization of oocytes by sperm; IVF or ICSI • Probably second best; oocyte cryopreservation after ovarian stimulation followed by oocyte retrieval
Ovarian stimulation is not suitable for certain cancer patients; no sufficient time and/or ovarian stimulation contraindicated Solution ? Trial: Retrieval of immature oocytes from unstimulated ovaries, and maturation in-vitro followed by cryopreservation of oocytes by vitrification
Viability and pregnancy outcome of vitrified IVM oocytes Chian et al, 2008, Fertil Steril, in press
Fertility preservation strategies offered for women at MRC with cancer Chemotherapy cannot be delayed and/or hormonal stimulation contraindicated Chemotherapy can be delayed and hormonal stimulation not contraindicated Ovarian wedge resection or oophorectomy Immature oocyte retrieval Ovarian stimulation mature oocyte retrieval Immature oocyte retrieval from ovarian tissue IVM Male partner available (ICSI) Male partner available No male partner available No male partner Ovarian tissue cryopreservation Embryo cryopreservation Embryo cryopreservation Ooycte vitrification Ooycte vitrification
Outcome of IVM, IVF, ICSI and normal pregnancies • obstetrical and perinatal outcome of 432 babies (55 IVM, 217 IVF, 160 ICSI) compared with 1,296 age-matched spontaneous pregnancies (controls) delivered at a single hospital (MUHC) Buckett et al. Obstet Gynecol 2007; 110:885-91
Relative risk for any congenital abnormality compared with controls
Pregnancy outcomes per clinical pregnancy after IVM, IVF and ICSI Buckett et al Fertil Steril 2007
Pregnancy Outcome in IVM • Mikkelsen et al. (2005) ----- 47 IVM babies • 2 twins • 1 NT Normal karyotype • 2 preterm deliveries • 1 stillbirth (42 weeks) • 1 chromozomal abnormality