Vastus Slide and Controlled Perforations
110 likes | 257 Vues
This instructional course chapter presents the Vastus Slide technique for revision total hip arthroplasty (THA). Given the increasing number of revision THAs and their complexity, the course emphasizes the importance of safe cement removal. The Vastus Slide technique allows for extensive femoral exposure while protecting neurovascular structures. Key surgical steps include precise incisions, maintaining abductor musculature integrity, and employing controlled perforations for optimal cement removal. This method preserves blood supply, enhancing postoperative recovery and outcomes for hip reconstructive procedures.

Vastus Slide and Controlled Perforations
E N D
Presentation Transcript
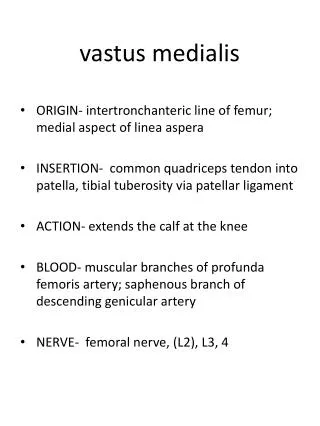
Vastus Slide and Controlled Perforations Instructional Course Lectures Chapter 3, Volume 48, 1999 Head, MD; Montgomery, MD; Emerson, MD Sepein Chiang, D.O.
Introduction • Increasing number of revision THA • More challenging and higher potential for complications than primary THA • Cement removal is one of the more difficult aspects • Vastus slide technique provides wide exposure and access to the femur • Controlled perforations offer a safe, expedient method for cement removal
Technique • Pt is placed in the lateral decubitus position • Patellae are used as guides for leg length • Access to both the femur and acetabulum • Can be extended both proximally & distally • Anterior to posterior access to the hip joint • Allows for sciatic nerve exploration • Follow anatomic planes to avoid potential for neurovascular injury
Technique (cont) • Incision begins 10-15 cm superior & slightly posterior to the greater trochanter • Incision carried distally along the femur below the level requiring cement removal • Skin, subcutaneous tissue, iliotibial band, gluteus maximus fascia • Lateral intermuscular septum remains intact and protects the sciatic nerve
Technique (cont) • Slide technique to the gluteus medius and vastus lateralis is done thru a lazy “Z” incision • A to B, A to D are carried out in a subperiosteal fashion • Periosteal dissection carried distally, reflecting the vastus lateralis and intermedius • B to C reflects the anterior portion of the gluteus medius & minimus
Technique (cont) • Avoid violating the abductor musculature • Superior gluteal nerve lies 4-5 cm above the greater trochanter between the gluteus medius and minimus • Externally rotate the hip and expose the hip capsule • Capsulectomy and dislocation
Technique (cont) • For cement removal the femur is externally rotated, knee flexed and the leg is dropped off the table • First removal the proximal lateral cement or run the risk of trochanteric fractures • Remove the femoral component
Technique (cont) • Midas-Rex pneumatic cutting tool to remove the cement • 5-7 cm distally, make a 7 mm perforation into the medullary canal with a Midas-Rex burr • For primary implants, 2 portals are usually sufficient
Technique (cont) • Portals are placed at least 5 cm apart • The distal portal is placed at least 2.5 cm proximal to the tip of the revision prosthesis • Portals allow the use of irrigation to remove cement debris
Conclusion • Differs from the Hardinge approach in that the substance of the abductor musculature is not invaded • Medial and posterior muscle attachments are maintained thereby preserving the blood supply to the femur • All reconstructive hip procedures can be accomplished through this surgical approach