Malnutrition
Malnutrition. Dr K N Prasad Community Medicine. “PEM”: Invariably reflects combined deficiencies in…. Protein : deficit in amino acids needed for cell structure, function Energy : calories (or joules) derived from macronutrients: protein, carbohydrate and fat


Malnutrition
E N D
Presentation Transcript
Malnutrition Dr K N Prasad Community Medicine
“PEM”: Invariably reflects combined deficiencies in… • Protein: deficit in amino acids needed for cell structure, function • Energy: calories (or joules) derived from macronutrients: protein, carbohydrate and fat • Micronutrients: vitamin A, B-complex, iron, zinc, calcium, others
OVERVIEW OF PEM • The majority of world’s children live in developing countries • Lack of food & clean water, poor sanitation, infection & social unrest lead to LBW & PEM • Malnutrition is implicated in >50% of deaths of <5 children (5 million/yr)
What is Malnutrition? • Both protein-energy malnutrition (underweight etc.) and micronutrient deficiencies • Retards physical and cognitive growth; increases susceptibility to infections • Cause of half of all child deaths, and more than half of deaths due to major diseases (malaria, diarrhea, pneumonia, measles) • Cause of 22% of disease burden of country
Underweight • Prevalence of underweight children is highest in the world, double of sub-Saharan Africa, more than a third of undernourished kids of the world live in India. • Most retardation occurs by age 2 (30% low birth weight)
EPIDEMIOLOGY • The term protein energy malnutrition has been adopted by WHO in 1976. • Highly prevalent in developing countries among <5 children; • severe forms 1-10% • underweight 20-40%. • All children with PEM have micronutrient deficiency.
PEM • In 2006 WHO estimated that 32% of <5 children in developing countries are underweight (182 million). • 78% of these children live in South-east Asia & 15% in Sub-Saharan Africa. • The reciprocal interaction between PEM & infection is the major cause of death & morbidity in young children.
"South Asian Enigma" • South Asian countries have worse incidence of malnutrition than Africa. • Characteristics of south Asia: low birth weight, less powerful women, poor sanitation.
PEM in Sub-Saharan Africa • PEM in Africa is related to: • The high birth rate • Subsistence farming • Overused soil, draught & desertification • Pets & diseases destroy crops • Poverty • Low protein diet • Political instability (war & displacement)
Causes for severe Malnutrition • Chronic, severely low energy and protein intake • •Exclusive breast feeding for too long • •Dilution of formula • •Unclean/non-nutritious, complementary foods of low energy and micronutrient density • •Infection (eg, measles, diarrhea, others) • •Xenobiotics (aflatoxins)
PRECIPITATING FACTORS • LACK OF FOOD (famine, poverty) • INADEQUATE BREAST FEEDING • WRONGCONCEPTSABOUT NUTRITION • DIARRHOEA & MALABSORPTION • INFECTIONS (worms, measles, T.B)
Anthropometric Measurements of Nutritional Status • Weight • Length/height • Mid upper arm circumference MUAC) • Chest circumference • Head circumference • Skin fold measurements: Triceps and Subscapular region
CLASSIFICATION • A. CLINICAL ( WELLCOME ) • Parameter: weight for age + oedema • Reference tandard (50th percentile) • Grades: • 80-60 % without oedema is underweight • 80-60% with oedema is Kwashiorkor • < 60 % with oedema is Marasmus-Kwash • < 60 % without oedema is Marasmus
CLASSIFICATION (2) • B. COMMUNITY (GOMEZ) • Parameter: weight for age • Reference standard (50th percentile) WHO chart • Grades: • I (Mild) : 90-70 • II (Moderate): 70-60 • III (Severe) : < 60
KWASHIORKOR Cecilly Williams, a British nurse, had introduced the word Kwashiorkor to the medical literature in 1933. The word is taken from the Ga language in Ghana & used to describe the sickness of weaning.
Kwashiorkor • Edema • Mental changes • Hair changes • Fatty liver • Dermatosis (skin lesions) • Infection • Moderate wasting • High case fatality • Low prevalence • 1st to 3rd years of life
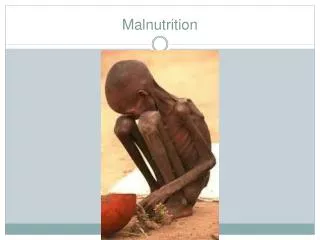
Marasmus • Severely wasted (emaciated) & stunted • Very much wasting • “Balanced” starvation • “Old Man” face, wrinkled appearance, sparse hair • No edema, fatty liver, skin changes • Too little breast milk or complementary foods • < 2 yrs of age
Prevention of PEM • Maintain nutritional status of infants and children at highest possible level. • Reducing risk and effects of infection • Nutritional health education: education of the mothers in the ante-natal care during pregnancy and after birth about the sound feeding and meaning during infancy.
TREATMENT • Correction of water & electrolyte imbalance • Treat infection & worm infestations • Dietary support: 3-4 g protein & 200 Cal /kg body wt/day + vitamins & minerals • Prevention of hypothermia • Counsel parents & plan future care including immunization & diet supplements
KEY POINT FEEDING • Continue breast feeding • Add frequent small feeds • Use liquid diet • Give vitamin A & folic acid on admission • With diarrhea use lactose-free or soya bean formula
Thought for the day An investment in knowledge always pay the best interest.