Download
1 / 28
410 likes | 1.63k Vues
Corneal Graft Rejection and Graft Failure. CORNEAL GRAFT FAILURE. PRIMARY GRAFT FAILURE REJECTION ´Khodadoust´ line rejection line: stromal oedema: INFECTION RAISED IOP DISEASE RECURRENCE DELAYED ENDOTHELIAL FAILURE WOUND DEHISCENCE (TRAUMA). Rejection of Solid Allografts,.

E N D
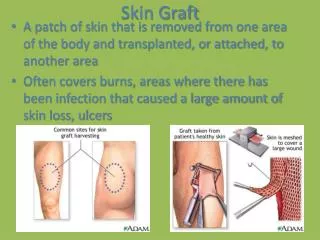
CORNEAL GRAFT FAILURE • PRIMARY GRAFT FAILURE • REJECTION ´Khodadoust´ line rejection line: stromal oedema: • INFECTION • RAISED IOP • DISEASE RECURRENCE • DELAYED ENDOTHELIAL FAILURE • WOUND DEHISCENCE (TRAUMA)
Rejection of Solid Allografts, • Classification • 1 Hyperacute- preformed antibody • 2 Acute- < 4 weeks Activation of T cell clones and destruction of graft by cytotoxic T cells • 3 Chronic -usually progressive arteriolitis refractory to immunosupressive therapy • Cornea =endothelial loss, mainly
Immune Privilege in the Eye • Dynamic process, actively maintained. (Kaplan) • Eye dependent modification of afferent and efferent limbs of the immune system • "Afferent block" • Blood eye barrier • Modified professional APC cells • Ocular fluids suppress compliment activation • ACAID (Strelein)
Factors which unfavourably regulate immune privilege • Langerhan's APC Cells • Neovascularisation
Corneal immunogenicity • Corneal immunogenicity is likely controlled by a multiplicity of factors, perhaps the most important of which is the human leukocyte antigen (HLA) system, which is the major histocompatibility complex in humans. • Four major loci on chromosome 6 code for the various tissue antigens. These loci have been designated HLA-A, B, and C (class I antigens) and HLA-DR (class II antigens). Class I antigens have been found on corneal epithelial, stromal, and endothelial cells,while Langerhans' cells, which are dendritic cells of mesenchymal origin located within the corneal epithelium, appear to be the primary cell type expressing class II antigens.Transient corneal cells of hematopoietic origin (primarily B lymphocytes and macrophages) may also express class II antigens.
MECHANISM OF CORNEAL GRAFT FAILURE • Type IV cell-mediated immune reaction. • Role of CD-4 cells: • Foreign MHC class II antigens act as a strong stimulus and can be recognized by host CD4+ T cells. The host Langerhans cells can also process foreign class I antigen and present it in conjunction with self-class II molecules to host CD4 T cells. The result of either mechanism is CD4 T-cell activation. Activated CD4 T cells release IL-2 and other lymphokines that stimulate the proliferation and activation of CD4 T cells, cytotoxic T cells, and B lymphocytes. • Role of CD-8 cells: • Host cytotoxic T cells (CD8+ ) can recognize foreign class I cell-surface antigens on the surface of donor cells. They result in lysis of the donor cells. NK activity also has a cytotoxic role. • B Lymphocytes • Antibody production by B cells enables opsonization, complement binding, and facilitation of antibody-dependent cell-mediated cytotoxicity (K cell activity). • Exaggerated response by induction of donor MHC class II • CD8 T cells modulate the response by releasing cytokines such as interferon IFN-g. This induces class II antigen expression on donor cells. Increased class II antigen expression creates a positive feedback loop on the cell-mediated allograft rejection.
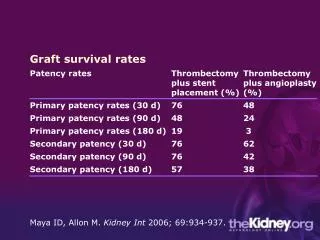
Survival Of PK (Coster) • 91% at 1 year • 75% 5 • 69% 7 • Loss is 35% at 1 year if corneal bed vascularised
The indications for penetrating keratoplasty • fall into the following four general categories: • optical • tectonic • therapeutic • cosmetic
Preparation of Cornea • McCarey-Kaufman, Optisol, or Dexsol media. Some surgeons prefer to harvest their donor tissue from a fresh whole globe, although this is becoming unfeasible given the time delay necessitated by required serologic testing of the donor for hepatitis B and C, human immunodeficiency virus infection, and syphilis.
Indications for PK • Keratoconus 30% • Bullous Keratopathy 25% • PreviousGraft18%
Graft Rejection • CLINICAL FEATURES • Decreased visual acuity, tearing, photophobia, • EPITHELIAL REJECTION • elevated epithelial rejection line, stains with fluoroscein and Rose Bengal, progresses across cornea over days to 3 weeks. Not serious as normally the button is resurfaced with host epithelial cells • SUBEPITHELIAL REJECTION • 0.2-0.5mm infiltrates beneath Bowman's with associated anterior chamber activityOften 10 months after surgery.
Subepithelial infiltrates • Subepithelial infiltrates are small, discrete opacities located immediately beneath the epithelium that may be seen diffusely scattered across the graft They are very similar in appearance to the subepithelial lesions present in epidemic keratoconjunctivitis. The lesions can be subtle and are often missed with a narrow slit lamp beam; they are best seen with a broad beam casting diffuse side illumination. Subepithelial infiltrates clear with topical corticosteroids but may leave a faint scar. They may be found at one time or another in about 15% of transplants and, like epithelial rejections, may be a sign of a generalized, low-grade, chronic immunologic reaction. We treat both epithelial rejection lines and subepithelial infiltrates with topical prednisolone sodium phosphate or acetate 1% every 3 hours while awake. The patient should return in 1 week, and, if improved, the drops are tapered by half every 3 days.
STROMAL REJECTION • sudden onset, full thickness haze and circumcorneal injection
ENDOTHELIAL REJECTION • ´Khodadoust´ line - a line of keratoprecipitates moving centrally across the cornea followed by endothelial cell destruction. • Mild-moderate anterior chamber activity and stromal oedema • May be diffuse reaction affecting entire cornea. • Severe resulting in later corneal stromal neovascularisation.
The signs of an endothelial rejection include- • The signs of an endothelial rejection include circumcorneal injection, an anterior chamber reaction, keratic precipitates present on the graft, an endothelial rejection line, and graft edema. The anterior chamber reaction is usually mild, frequently with no more than 1+ cell or flare. The keratic precipitates may be diffusely scattered or grouped or may form an irregular line of precipitates (Khodadoust line) that begins at the graft periphery, often near an area of vascularization or synechial formation, and then progresses over the endothelial surface of the donor tissue, leaving in its wake a decompensated, edematous graft . • Histologically, lymphocytes are seen adherent to the endothelial surface, often separating destroyed endothelium from normal-appearing endothelial cells.
IMMUNE PRINCIPLES OF GRAFT REJECTION • TREATMENT • Topical steroids sufficient for more anterior rejection • Oral prednisolone tapering over 2 weeks if poor response to topical treatment or endothelial rejection • Cyclophosphamide / azathioprine / cyclosporin A
Other Complications • Many other complications can occur in the late postoperative period, some of which are peculiar to corneal transplant surgery and others of which may be seen after any intraocular surgery. Chronic progressive nonspecific endothelial decompensation manifests as a gradual onset of graft edema secondary to endothelial dysfunction not associated with prior rejection, uveitis, or glaucoma. Recurrence of host disease in the graft may be seen in several situations. Herpes simplex keratitis can frequently recur in the graft, whereas bacterial keratitis is far less common. Several of the corneal dystrophies may recur after penetrating keratoplasty, with Reis Buckler Reis-Bücklers' dystrophy being the most common. • Among the stromal dystrophies, lattice dystrophy recurs more frequently than either granular or macular dystrophy.
HSV- graft survival • HSV- graft survival = 70% at 3 yearsCover post operatively with oral acyclovir / topical acyclovir in conjunction with the steroid drops.Corneal grafts affected by recurrent Herpes simplex have a typical appearance because the disease occurs at the graft interface (the cut ends of the corneal nerves presumably release virus at this location).
GRAFT INFECTIONS • HSV- graft survival = 70% at 3 yearsCover post operatively with oral acyclovir / topical acyclovir in conjunction with the steroid drops.Corneal grafts affected by recurrent Herpes simplex have a typical appearance because the disease occurs at the graft interface (the cut ends of the corneal nerves presumably release virus at this location). • HZO- poor candidates for grafts as decreased sensation, lid abnormalities, vascularisation, uveitis, glaucoma • Bacterial / fungal- source from donor tissue, host tissue and environment • Increased risk if loose sutures, steroids, KCS, HSV • Acanthamoeba- primary or recurrent infection in graft. Suspect if poor response to usual antibiotic Rx
PRIMARY DONOR FAILURE • Irreversible graft oedema occurring in immediate post-op period • Due to :- • inadequate or prolonged corneal preservation, poor graft material, surgical trauma • effect of IOL • semiflexible closed loop A/C IOL or • iris supported IOLs have an increased incidence of graft failure.
GLAUCOMA • May be pre-existing, aphakia, pseudophakia, PAS, A/C IOL related, • viscoelastic related
Transmission of donor disease to the host may occur and can be serious or even life threatening. Reports in the literature on transplantation of infected donor tissue into previously healthy recipients reveal cases of bacterial endophthalmitis, fungal endophthalmitis,fungal keratitis, and bacterial keratitis. Transmission of rabies into four patients and Creutzfeldt-Jakob disease in one patient have led to the death of each recipient. Corneal tissue from five donors who at the time of their death were not known to be infected with the human immunodeficiency virus (HIV) has been transplanted into 10 healthy recipients. Serial antibody testing for HIV has not shown conversion from negative to positive in the recipients over a period of at least 130 days. One recipient has refused HIV testing but has remained healthy and symptom-free over a period of several years. Long-term follow-up of these individuals will determine whether HIV antibody seroconversion or development of the full acquired immunodeficiency syndrome may occur from transplantation of infected donor tissue. Transmission of donor disease
Transmission of donor disease • Corneal donors are tested for hepatitis B and C, syphilis, and HIV infection. Positive tests preclude the use of this donor tissue for transplantation
CJD and the Eye • Creutzfeld-Jakob Disease (CJD) is a frightening but nonetheless intriguing disease. It occurs in most populations at approximately 1 case per million per year. It is referred to as classical or sporadic CJD to disitnguish it from new variant CJD (nvCJD) of which there have been to date a total of 25 cases and which is thought to be the human equivalent of bovine spongiform encephalopathy (BSE). Classical CJD is not contagious but has been transmitted by transplantation of cornea 1 (world total of 3 cases), dura mater, pituitary growth hormone and by comtaminated neurosurgical instruments and cortical electrodes. Although there is rapidly progressive dementia invariably leading to death usually within months of onset, it is a diagnosis that is only confirmed postmortem by characteristic spongiform change or immunochemical identification of the pathological isoform of the prion protein in the brain. Although it has long been an absolute contraindication to corneal donation its exclusion can only be achieved by a low threshold of suspicion as there is as yet no serological screening test.
Eye Banking and Audit • All consultant ophthalmic surgeons who undertake ocular tissue transplantation should have knowledge of the procedure of eye procurement and banking, understand the unique risks involved and accept that they have ultimate responsibility for their patients who should be well informed. • All Medical Directors of Eye Banks should ensure that all ocular tissue is traceable to its destination. This includes tissue that is used in research or is discarded as unsuitable or surplus to requirement in addition to that used in recipient patients. • All consultant ophthalmologists and their junior staff who undertake transplantation of any kind should actively take part in routine long term follow-up of clinical outcome. Revised forms for transplant, six month and annual follow-up thereafter are currently being evaluated.
Action So Far • After receiving expert advice from the Spongiform Encephalopathy Advisory Group in December 1997, all surgeons offered the three patients explantation of ocular tissue. Two patients accepted the advice and had further surgery by January 1998. All three remain well. • The Duty Office at UKTSSA now routinely asks if a postmortem on a donor is pending. No tissue is issued form the CTS Banks in Bristol and Manchester until such time as the result is known (December 1997). • The CTS Eye Bank policy on sclera has been changed to ensure that sclera cannot be held in stock and that sclera from any single eye is not transplanted into more than one individual and can always be traced to a named recipient (i.e. a policy which is in line with corneal transplantation) • Sir William Stewart chaired an expert group who undertook and subsequently published on behalf of the governemnt (April 1998) an independent review of the incident which contains recommendations. Copies can be obtained from Margaret Hallendorff at the College. • Guidelines for retrieval of donor eyes have now been accepted by the College and are available, including on this website. All ophthalmic units are expected to have read this document. • A re-designed ocular tissue donor information form and contrainidication list are now issued with UKTSSA retrieval boxes (July 1998).
Ocular Tissues Standards and Audit Group (OTSAG) • The recommendations of the Stewart report are under active consideration principally by the Ocular Tissues Standards and Audit Group (OTSAG). This Group was established in 1996 and seeks to define essential and best practice in the fields of ocular and non-ocular tissue transplantation. The following proposals are currently under consideration: • The Royal College of Ophthalmologists should develop a portfolio of documents defining standards in the transplantation of the cornea, sclera and all other ocular and non-ocular tissues into the human eye. • The portfolio should be compiled and updated by OTSAG which is accountable to the Royal College of Ophthalmologists and to the Corneal Advisory Group at UKTSSA. • All units regularly undertaking ocular tissue transplantation should contribute to the supply of ocular tissue for transplantation and research nationwide.