Download
1 / 39
450 likes | 894 Vues
GES 107 Introduction to Epidemiology of HIV and AIDS. Georgina N. Odaibo and Prof Olaleye Department of Virology COM, UI. Definitions. VIRUS A virus is the smallest known infective agent. They are also known as ‘filterable agent’

E N D
GES 107Introduction to Epidemiology of HIV and AIDS Georgina N. Odaiboand Prof Olaleye Department of Virology COM, UI
Definitions • VIRUS • A virus is the smallest known infective agent. • They are also known as ‘filterable agent’ • Depend absolutely on the mechanisms of host cells for survival. • Outside the host, a virus is inert i.e they are non-living. • Unlike other organism that possess both RNA and DNA, the genetic material of viruses are either DNA or RNA. • Not every virus will infect every cell; they have affinity for specific host cell. • For example HIV has affinity for CD4 bearing cells • Hepatitis B virus has affinity for hepatocytes of the liver.
AIDS • Acquired Immunodeficiency Syndrome. • Acquired • means that the disease is not hereditary but from contact with a disease-causing agent (in this case, HIV). • Immunodeficiency • means that the disease is characterized by a weakening of the immune system. • Syndrome • refers to a group of symptoms that indicate or characterize a disease.
HIV • Acronym for the Human Immunodeficiency virus, the • virus that causes acquired immunodeficiency syndrome (AIDS). • It is a retrovirus that has an RNA genome and a reverse transcriptase enzyme. • The usual direction of flow of genetic material is DNA →RNA • but retroviruses can go from RNA→DNA with the aid of the reverse transcriptase (RT)enzyme • The viral DNA integrates itself into the DNA of the host and then take over the activity of the cell.
Difference B/W HIV and AIDS • AIDS is the late stage of HIV infection – the presence of clinical disease • HIV infected – the virus is present in the body • Not everyone that is infected with HIV that has AIDS • Most HIV infected individuals will develop AIDS if not on anti-retroviral drugs
Diagram of Human Immunodeficiency Virus-1 Function of HIV proteins Gp 120: part of envelope- for attachment of virus to cell Gp41: part of envelope- used to internalize virus into cell Lipid Membrane: envelope provides external covering to the virus Integrase: enzyme used to integrate virus genome to host genome Reverse transcriptase: enzyme used to convert viral RNA to viral cDNA that gets integrated into the host genome Viral RNA: Genome of the virus Capsid: protein that surrounds the genome/nucleic acid
HIV TYPES AND SUBTYPES • HIV is a highly variable virus which mutates very readily/easily • This means there are many different strains of HIV, even within the body of a single infected person. • Based on genetic similarities and differences, HIV has been classified into two types, HIV-1 and HIV-2. • Both types are transmitted through the same mode and appear to cause clinically indistinguishable AIDS. • Worldwide, the predominant virus is HIV-1 • HIV-2 type is concentrated in West Africa and among those who has lived or interacted with those from West Africa
HIV Subtypes • HIV types are classified into groups which are further classified into subtypes. • HIV-1 can be classified into four groups: the "major" group M, the "outlier" group O and two new groups, N and P. • More than 90 percent of HIV-1 infections belong to HIV-1 group M. • Within group M, at least nine genetically distinct subtypes(or clades) of HIV-1 have been identified. • These include subtypes A, B, C, D, F, G, H, J and K.
Subtypes cont. • HIV-1 also has unique property of recombination • the ability of fragment of two or more subtypes to come together and form a mosaic strain known as ‘circulating recombinant form (CRF). • E.g. the CRF 02 which was first isolated in Ibadan by Olaleye et al is a mixture of subtypes A and G • The AG recombinant, alsoknown as IbNg (Ib-Ibadan Ng-Nigeria) is the predominant subtype circulating widely in West and Central Africa.
Genomic structure of a circulating recombinant form (CRF02_AG)
Global Distribution of HIV Subtypes • Subtype B predominates in the Americas, Western Europe and Australia • Subtype C, a mixture of B, C, and BC recombinants predominates in Asia • Africa shows the greatest diversity of circulating HIV subtypes and recombinants. • Subtype C dominates the South and East (A and D also present) • West and West Central Africa harbor mainly CRF02_AG, alongside a complex array of other recombinants each present at a low frequency • The most complex epidemic is in Central Africa, where rare subtypes and a wide variety of recombinant forms circulate without any distinct predominant strain
HIV-2 Subtypes • There are 8 known HIV-2 subtypes (A to H). • only groups A and B are epidemic. • Group A spreads mainly in West Africa, but also to Angola, Mozambique, Brazil, India and rarely to Europe or the US. • Group B is mainly confined to West Africa
HIV Type 1 Type 2 N (Non-M non-O) M (Major) O (Outliers) A B C D F G H J K >49 CRFs A B C D E F G H P HIV CLASSIFICATION
Infection with one particular HIV type or subtype does not protect against infection with other type/subtypes • i.e multiple infection do occur • New HIV genetic subtypes and CRFs • may be discovered in the future • current subtypes and CRFs will also continue to spread to new areas as the global epidemic continues.
HOW HIV CAUSES AIDS • HIV infects and destroys cells of the immune system known as T-helper cells (CD4 bearing cells) • The immune system is the arm of the body that defends and protects the body against infection • The T-helper cells are the most important cells of the immune system; they play a central role, coordinating the activities of other cells involved in the immune response • There is a protein molecule on the surface of the T-helper cells known as CD4 hence the T-helper cells are also known as CD4 bearing cells (CD4+).
Diagrammatical representation of the critical role of T4 Lymphocyte in the Human Immune Response
How HIV causes AIDS cont. • Once the virus enters the cells • it replicates in it and eventually destroys the cell, • many virus particles are released which in turn infects other T-helper cells and the cycle continues • As the virus destroys the CD4 cells • Initially, the body replaces them (long incubation period, asymptomatic stage, clinical latency) • their number reduces gradually to a point that the cells are not enough to carry out their function of defending the body effectively. • The amount of virus circulating in the blood increases as the CD4 cells decreases • At this point, opportunistic infections set in and this individual is said to have developed AIDS
Virus and CD4 levels over the course of an untreated HIV infection
CD4 Count, Viral Load and Clinical Course Primary Infection Sero-conversion Intermediate Stage AIDS CD4 Cell Count Viral Load 1,000 CD4 Cells 500 4-8 Weeks Up to 12 Years 2-3 Years
People who are not infected with HIV and generally are in good health have roughly 700 to 1,200 CD4+ T cells per microliter. • This range varies by geographic location, race and by age. • In Nigeria, the CD4+ cell ranges from 365 to 1571 cell/ul in adults and 750 to 3000 cells/ul in children bellow 12 years.
Opportunistic infections • infections that take advantage of the opportunity offered by a weakened immune system to cause disease • These are diseases that people with healthy immune systems can also get, but with HIV they occur at a much higher rate. • It also takes longer for a person with HIV to recover from these diseases than it takes for someone with a healthy immune system. • When the immune system is very weak due to advanced HIV disease or AIDS, some opportunistic infections can spread to a number of different organs • This is known as 'disseminated' or 'systemic' disease. • Many of the opportunistic infections that occur at this late stage of HIV infection can be fatal. • Opportunistic infection may be caused by viruses, bacteria, fungi or parasites. A partial list of the world's most common HIV-related opportunistic infections and diseases includes:
Opportunistic infections cont. • Bacterial diseases such as • tuberculosis, Mycobacterium Avium Complex (MAC), bacterial pneumonia and septicaemia (blood poisoning) • Protozoal diseases such as • toxoplasmosis, microsporidiosis, cryptosporidiosis, isopsoriasis and leishmaniasis • Fungal diseases such as • PneumonisticCarini pneumonia (PCP), candidiasis, cryptococcosis and penicilliosis • Viral diseases such as • those caused by cytomegalovirus, herpes simplex and herpes zoster virus • HIV-associated malignancies such as • Kaposi's sarcoma, lymphoma and squamous cell carcinoma. • Tuberculosis is the number one opportunistic infection in Africa.
CLINICAL SYMPTOMS OF AIDS The following may be indication of advanced HIV infection: • rapid weight loss • dry cough • recurring fever • profuse night sweats • profound and unexplained fatigue • swollen lymph glands in the armpits, groin, or neck • diarrhea that lasts for more than a week • white spots or unusual blemishes on the tongue, in the mouth, or in the throat • pneumonia • red, brown, pink, or purplish blotches on or under the skin or inside the mouth, nose, or eyelids • memory loss, depression, and other neurological disorders Each of these symptoms can be related to other illnesses. Thus the only way to determine whether one is infected is to be tested for HIV infection using laboratory techniques.
DIAGNOSIS OF HIV INFECTION • The effective control of HIV in any country must among other measures depend on the establishment and provision of accurate and reliable diagnostic techniques. • The presence of HIV in the body courses the immune system to react and produce a substance called antibodies. • Routine diagnosis of HIV infection is based mainly on detection of these HIV specific antibodies in the blood. • Because the diagnosis of HIV infection in a particular person requires a high degree of both sensitivity and specificity, the testing is done in two stages • screening and then confirmation.
Screening • High Sensitivity (Negative truly negative) • Antibody detection • Specific HIV antibodies • ELISA technique • RAPID ASSAYS-agglutination, immunodot (dipstick) etc. • Blood/saliva/urine specimen could be used • Best result obtained with blood samples
CONFIRMATORY ASSAYS High Specificity (Positive truly positive) • Antibody Detection • WB, IFA etc • Antigen Detection • Detection of viral antigen-p24-ELISA • Virus isolation-Cell culture • Detection of viral nucleic acid-PCR
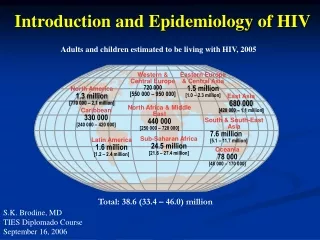
EPIDEMIOLOGY OF HIV • In 2009, there were an estimated 2.6 million (1.8 million in sub-Saharan Africa) people who became newly infected with HIV (UNAIDS, 2010) • Estimated 33.3 million people (22.5 million in sub-Saharan Africa) living with HIV in 2009 (UNAIDS, 2010). • AIDS has caused death of an estimated 25 million people by 2007 (UNAIDS, 2008). • Estimated 1.8 million people (1.3 million in sub-Saharan Africa) including about 260,000 children died of AIDS pandemic in 2009 alone (UNAIDS, 2010). • Responsible for one in five deaths in sub-Saharan Africa (UNAIDS and WHO, 2002). • About two-thirds (68%) of all people living with HIV reside in sub-Saharan Africa (UNAIDS, 2010)
The HIV Situation in Nigeria • Nigeria has the third-largest number of people living with HIV in the world • The HIV epidemic in Nigeria is complex and varies widely by region • The prevalence in the general population is determined by a • National HIV sentinel survey among women attending antenatal clinics in both the rural and the urban areas of the country • The sentinel survey is repeated every two years in all states of the Federation and FCT • In some states, the epidemic is more concentrated, while other states have more generalized epidemics • The reason for the difference in the rate of infection is not very clear, though some researchers have attributed it to difference in sexual behaviour.
Fig:7 Geographical Distribution of HIV Prevalence by States in Nigeria (FMOH, 2010)
Nigeria situation cont. • The first cases of HIV and AIDS in Nigeria were reported in 1986 • The prevalence of the virus increased from 1.8% in 191 when the first sentinel survey was conducted to a peak of 5.8% in the 2001 survey and then a drop to 5.0% in 2003 • 2010 survey showed that the National prevalence has stabilized at about 4.0% • Estimated 3.1 million adults are living with HIV
Nigeria situation cont. • The main HIV transmission routes • heterosexual sex which constitutes 90-95%, • blood transfusions (2nd largest) • and mother-to-child-transmission • injection drug use and homosexual sex are accounting for an increasing number of new HIV infections hence their role in the spread of the virus is becoming very important in Nigeria. • Study in Lagos report 45% among men having sex with men (MSM)
Nigeria situation cont. • @ beginning- male to female ratio was approximately 1:1 • recent data has shown that the rate is higher in women (56%) • Youth and young adults in Nigeria are particularly vulnerable to HIV • rate consistently high among 15-24 years
Nigeria situation cont. • Major support on HIV/AIDS • USG Presidents Emergency Plan for AIDS Relieve (PEPFAR) • Global fund • World Bank • FGN