Download
1 / 22
220 likes | 368 Vues
The Scott & White Family Caregiver Program: Implementing the REACH II Intervention Components in a Healthcare Setting. Alan B. Stevens Vernon D. Holleman-Lewis M. Rampy Centennial Chair in Gerontology Scott & White Healthcare. The Scott & White Family Caregiver Program.

E N D
The Scott & White Family Caregiver Program: Implementing the REACH II Intervention Components in a Healthcare Setting Alan B. Stevens Vernon D. Holleman-Lewis M. Rampy Centennial Chair in Gerontology Scott & White Healthcare
The Scott & White Family Caregiver Program • First two years funded by the Johnson & Johnson/ Rosalyn Carter Institute Caregivers Program (Phase I) • Now funded by Scott & White Healthcare (Phase II)
Our Approach • Use implementation research methods to embed an evidence-based intervention for family caregivers (Resources for Enhancing Alzheimer’s Caregiver Health II -- REACH II) • Leverage characteristics of an integrated healthcare system to target, identify, and enroll family caregivers in need of support • Deliver and evaluate the innovative support program on caregiver quality of life indicators • Position the program as an asset to Scott & White’s Mission and Vision
Accomplishments of Phase I • Implemented an evidence based program in a limited number of primary care clinics and in Scott and White Memorial Hospital in Temple • Created A Caregiver’s Notebook that translates REACH II intervention materials • Enrolled 164 family caregivers in a 6 month program of support • Obtained financial support from expansion of program
Identification of Caregivers:Prompts embedded in Admission Documentation • Inserted a question regarding Alzheimer’s/Dementia in the Past Med/SurgHxscreen • Staff development around completion of questions • Only answer “yes” if patient or family member (or both) has a documented diagnosis of Alzheimer’s disease or other dementia (not for altered mental status only) • Follow up with care question
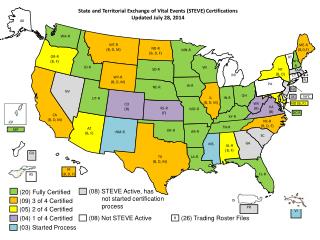
3,295 Alzheimer’s/dementia patients identified in hospital/clinic 2,561 – Not eligible Did not have a CG identified Not identified on eligible floor 734 Alzheimer’s/dementia patients with CG 265 – Not approached 469 Eligible patients given CG packet 54 – No CG contact 188 – CG packet not returned 59 – Declined 4 – Patient died 164 Caregivers enrolled: 84-Low; 75-Medium; 5-High 25 – Cancelled 7 – Transferred to CLP 25 – Lost to follow-up 35 – Did not return 6 month RAM 72 – Completed 6 month questionnaire Phase I Recruitment
Phase I Summary Findings • Significant decrease in overall caregiver risks reported by caregivers • No “high-risk” caregivers at 6 month follow-up • Significant questions indicate reduction in caregiver stress, burden, and safety 2009 Rosalynn Carter Leadership in Caregiving Award
Phase II Goals • To expand the Family Caregiver Program into other Scott & White Healthcare delivery settings • Conduct a cluster randomization trial with the REACH II Quality of Life measure as the main outcome measure • Continue program in Phase I sites (i.e., skills training and support intervention) • Randomize two additional service regions • 1 skills training and support intervention • 1 education group comparison
Skills Training and Support Intervention • 6 month intervention • Baseline Risk Assessment Measure/ REACH II Quality of Life • Create Family Profile and provide A Caregiver’s Notebook • 4 planned and 2 optional home visits • 6 month Risk Assessment Measure/ REACH II Quality of Life/ Satisfaction Survey
Education Group Components • 6 month intervention • Baseline Risk Assessment Measure/ REACH II Quality of Life • Provide educational packet • 2 check-in phone calls • 6 month Risk Assessment Measure/ REACH II Quality of Life/ Satisfaction Survey
FCP Tool Used to Promote Fidelity • Microsoft Access database • Uses a series of forms, tables and reports to track the progress of the intervention and log all interactions that occur between the patient and program staff • Used to evaluate both intervention implementation and outcomes
Phase II Recruitment to Date 438 Referrals to Family Caregiver Program Ineligible: 64 Admitted/Discharged to NH 75 Discharged before approached 29 No Caregiver 132 No qualifying diagnosis 13 Reside outside of service area 19 Other Tx Regions 1 & 2: 340 Ed Region: 98 106 Eligible Caregivers Not Enrolled: 10 Declined 43 Unresponsive 27 Other Tx Regions 1 & 2: 85 Ed Region: 21 26 Caregivers Enrolled Did not Complete: 1 Lost to Follow Up 1 Withdrew 6 Other Tx Regions 1 & 2: 19 Ed Region: 7 18 Completed Baseline QoL Tx Regions 1 & 2: 12 Ed Region: 6
Ongoing strategies to promote implementation and sustainability • Recruitment • Continue healthcare-based recruitment strategies (e.g., incentives, presentations, integration into other initiatives) • Expand recruitment to community partners (e.g., Area Agencies on Aging, Alzheimer’s Association chapters) • Align with other evidence-based health intervention initiatives • Assess the “value added” proposition • Identify the best “home” for the program
Special Thanks from Scott & White Healthcare to our Partners



![A B = 4 m b ln (d max /d min ) / [ r (d max – d min )]](https://cdn2.slideserve.com/4322513/slide1-dt.jpg)