Download
1 / 119
1.21k likes | 1.46k Vues
Acute and chronic meningitis, encephalitis III. Assoc Prof Dr Meral Sonmezoglu Yeditepe University Hospital.

E N D
Acute and chronic meningitis, encephalitis III Assoc Prof Dr Meral Sonmezoglu Yeditepe University Hospital
The two major divisions in the nervous system are the central nervous system (CNS), composed of the brain and the spinal cord, and the peripheral nervous system (PNS), composed of afferent (input to CNS) and efferent (output to periphery) neurons. Within the PNS, major divisions are the somatic nervous system (controls skeletal muscle) and in the autonomic nervous system, which has two branches: the parasympathetic (rest anddigest) and the sympathetic (emergency) branches.
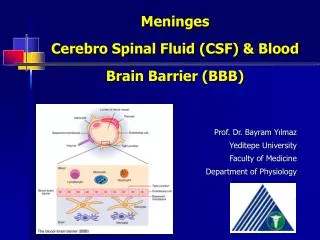
Protection of the Brain The brain is protected by bone, meninges, and cerebrospinal fluid (CSF)
The CSF circulates through the ventricular system • CSF is produced by the choroid plexus inside the ventricles. • It circulates through the ventricles. • From the fourth ventricle, CSF enters thesubarachnoid space, between thearachnoid mater and pia mater. • Reabsorbed from subarachnoid space into venous blood via the arachnoid villi
Meninges (s. meninx) Three connective tissue membranes external to the CNS – dura mater, arachnoid mater, and pia mater Functions: Cover and protect the CNS Protect blood vessels and enclose venous sinuses Contain cerebrospinal fluid (CSF) Form partitions within the skull
Dura Mater Tough meninx composed of two fibrous CT layers. Layers separate in certain areas and form dural sinuses. Dural sinuses collect venous blood from the brain. 3 dural septa limit excessive movement of the brain Falx cerebri – dural fold that dips into the longitudinal fissure Falx cerebelli – runs along the vermis of the cerebellum Tentorium cerebelli – horizontal fold extending into the transverse fissure
Arachnoid Mater Separated from the dura mater by the subdural space (a narrow serous cavity) Beneath the arachnoid is a wide subarachnoid space filled with CSF and large blood vessels Arachnoid villi protrude superiorly and permit CSF to be absorbed into venous blood
Pia Mater Deepest meninx – delicate CT that clings tightly to the brain and follows convolutions
Cerebrospinal Fluid (CSF) Watery, similar in composition to blood plasma, but contains less protein and different ion concentrations than plasma Forms a liquid cushion that gives buoyancy to the CNS organs, prevents the brain from crushing under its own weight Protects the CNS from blows and other trauma Nourishes the brain and may carry chemical signals from one part of the brain to another
Choroid Plexuses Clusters of interwoven capillaries in each ventricle between the pia mater and a layer of ependymal cells. Ion pumps allow them to alter the ion concentrations of the CSF Help cleanse CSF by removing wastes
Blood-Brain Barrier Protective mechanism that helps maintain a stable environment for the brain Bloodborne substances in brain capillaries are separated from neurons by: Continuous endothelium of capillary walls Relatively thick basal lamina Bulbous feet of astrocytes Least permeable capillaries in the body due the nature of the tight junctions between endothelial cells
Blood-Brain Barrier: Functions Selective barrier that allows nutrients to pass freely Is ineffective against substances that can diffuse through plasma membranes (fats, gasses, alcohol) Absent in some areas (vomiting center and the hypothalamus), allowing these areas to monitor the chemical composition of the blood
Meningitis Meningitis is a clinical syndrome characterized by inflammation of the meninges
Classification • Depending on theduration of symptoms, meningitismay be classified as acuteorchronic. • Acutemeningitisdenotestheevolution of symptomswithinhourstoseveraldays, whilechronicmeningitis has an onsetandduration of weekstomonths. • Theduration of symptoms of chronicmeningitis is characteristicallyat least 4 weeks.
Classification • Meningitis can also be classified according to its etiology.
Meningitis • Bacterial • Viral ( aseptic) • TB • Fungal • Chemical • Parasitic • ? Carcinomatous
Classification of Meningitis • Infectious • Bacterial • Viral • Fungal • Non-infectious • Drug-Induced • Neoplastic • Autoimmune
Bacterial Meningitis in Adults • Deeks SL. Bacterial meningitis in Canada (1994-2001). Canadian Communicable Disease Report. Dec 2005. 31:23.
Meningitis • Aseptic meningitis is a broad term that denotes a non-pyogenic cellular response, which may be caused by many different etiologic agents • Many of these cases are found to have a viral etiology and can then be reclassified as acute viral meningitis (eg, enterovirus meningitis, herpes simplex virus [HSV] meningitis).
BacterialMeningitis • Definition • Bacterial meningitis is an inflammatory response to bacterial infection of the pia-arachnoid and CSF of the subarachnoid space • Epidemiology • Incidence is between 3-5 per 100,000 • More than 2,000 deaths annually in the U.S. • Relative frequency of bacterial species varies with age.
Meningitis • Epidemiology • Neonates (< 1 Month) • Gm (-) bacilli 50-60% • Grp B Strep 20-40% • Listeria sp. 2-10% • H. influenza 0-3% • S. pneumo 0-5%
Meningitis • Epidemiology • Children (1 month to 15 years) • H. influenzae 40-60% • Declining dramatically in many geographic regions • N. meningitidis 25-40% • S. pneumo 10-20%
Meningitis • Epidemiology • Adults (> 15 years) • S. pneumo 30-50% • N. Meningitidis 10-35% • Major cause in epidemics • Gm (-) Bacilli 1-10% • Elderly • S. aureus 5-15% • H. influenzae 1-3% • >60 include Listeria, E. coli, Pseudomonas
Meningitis • Pathogenesis • Majority of cases are hematogenous in origin • Organisms have virulence factors that allow bypassing of normal defenses • Proteases • Polysaccharidases
Meningitis • Pathology and Pathogenesis • Sequential steps allow the pathogen into the CSF • Nasopharyngeal colonization • Nasopharyngeal epithelial cell invasion • Bloodstream invasion • Bacteremia with intravascular survival • Crossing of the BBB and entry into the CSF • Survival and replication in the subarachnoid space
Pathophysiology of Bacterial Meningitis • Bacterial colonization within the subarachnoid space • Initiation of inflammatory response which leads to: • Endothelial damage • Disruption of the blood-brain barrier • On a larger scale, this results in: • Cerebral edema • Cytotoxic • Vasogenic • Interstitial • Increased ICP
Meningitis • Pathology and Pathogenesis • Key advances in the pathophysiology of meningitis include the pivotal role of cytokines (eg, tumor necrosis factor-alpha [TNF-alpha], interleukin [IL]–1), chemokines (IL-8), and other proinflammatory molecules in the pathogenesis of pleocytosis and neuronal damage during bacterial meningitis. • Increased CSF concentrations of TNF-alpha, IL-1, IL-6, and IL-8 are characteristic findings in patients with bacterial meningitis
Meningitis • Pathology • Hallmark • Exudate in the subarachnoid space • Accumulation of exudate in the dependent areas of the brain • Large numbers of PMN’s • Within 2-3 days inflammation in the walls of the small and medium-sized blood vessels • Blockage of normal CSF pathways and blockage of the normal absorption may lead to obstructive hydrocephalus
Meningitis • Overall, the net result is vascular endothelial injury and increased BBB permeability leading to the entry of many blood components into the subarachnoid space. • This contributes to vasogenic edema and elevated CSF protein levels. • In response to the cytokines and chemotactic molecules, neutrophils migrate from the bloodstream and penetrate the damaged BBB, producing the profound neutrophilic pleocytosis characteristic of bacterial meningitis.
Pathophysiology of Bacterial Meningitis Complications: • Seizures • Hydrocephalus • Infarction • Herniation • From van de Beek D Community-acquired bacterial meningitis in adults. 354:1. 44.
ClinicalPresentation of Meningitis • Classicsigns ; • fever, headache, neckstiffness, photophobia, nausea, vomiting, andsigns of cerebraldysfunction (eg, lethargy, confusion, decreased level of consciousness coma). • Thetriad of fever, nuchalrigidity, andchange in mentalstatus is found in onlytwothirds of patients • Atypicalpresentationmay be observed in certaingroups (elderly, diabetic, neutropenic, immunocompromisedhosts..).
ClinicalPresentation of Meningitis • Signs of cerebral dysfunction are common, including confusion, irritability, delirium, and coma. These are usually accompanied by fever and photophobia. • Signs of meningeal irritation are observed in only approximately 50% of patients with bacterial meningitis, and their absence certainly does not rule out meningitis
Meningitis • Clinical Manifestations – Nuchal rigidity • Kernig’s • Pt supine with flexed knee has increased pain with passive extension of the same leg • Brudzinski’s • Supine pt with neck flexed will raise knees to take pressure off of the meninges • Present in 50% of acute bacterial meningitis cases • Cranial Nerve Palsies • IV, VI, VII • Seizures
Amos’s Sign Hips & knees flexed Back arched Neck in extension Trunk supported by arms
Meningitis • Focal neurologic signs may develop as a result of ischemia from vascular inflammation and thrombosis • Papilledema and other signs of increased ICP may be present. • Coma, increased blood pressure with bradycardia, and cranial nerve III palsy may be present. • The presence of papilledema also suggests a possible alternate diagnosis (eg, brain abscess).
Meningitis • Papilledema
Meningitis • Clinical Manifestations - Meningococcemia • Prominent rash • Diffuse purpuric lesions principally involving the extremities • Fever, hypotension, DIC • History of terminal complement deficiency • Classic findings often absent • Neonates • Elderly
Diagnosis of Meningitis • Diagnosis • Assess for increased ICP • Papilledema • Focal neurologic findings • Defer LP until CT scan or MRI obtained if any of above present • If suspect meningitis and awaiting neuroimaging • Obtain BC’s and start empiric Abx
Diagnosis of Meningitis Obtain CT scan before lumbar puncture in patients with: • Immunucompromised state • History of CNS disease • New onset seizures • Papilledema • Altered level of consciousness • Focal neurologic signs
Diagnosis of Meningitis • Obtain blood cultures and give empiric antibiotics if LP is delayed