Download
1 / 65
650 likes | 1.03k Vues
SERVING THE RETURNING VETERAN: THE POLYTRAUMA SYSTEM OF CARE . Andrea Karl, MD Ellen Kessi, MSW LCSW Katherine Noonan, Ph.D. Katrell Rhinehart, PT Kiersten Smith, MOTR/L Tricia Strombom, RN BSN. AGENDA. Background on Veterans Served TBI Primary Screen and Secondary Screening

E N D
SERVING THE RETURNING VETERAN: THE POLYTRAUMA SYSTEM OF CARE Andrea Karl, MD Ellen Kessi, MSW LCSW Katherine Noonan, Ph.D. Katrell Rhinehart, PT Kiersten Smith, MOTR/L Tricia Strombom, RN BSN
AGENDA • Background on Veterans Served • TBI Primary Screen and Secondary Screening • Polytrauma System of Care • Therapies Available within Polytrauma Clinic • Additional Resources
POLYTRAUMA TEAM • Andrea Karl, MD- Director of Polytrauma Clinic • Katherine Noonan, Ph.D.- Polytrauma Psychologist • Ellen Kessi, LCSW- Social Work Case Manager • Katrell Rinehart, PT-Physical Therapist • Kiersten Smith, MOTR/L-Occupational Therapist • Tricia Strombom, RN BSN- Nurse Case Manager
BACKGROUND ON VETERANS SERVED Tricia Strombom, RN BSN Polytrauma OEF/OIF Nurse Case Manager
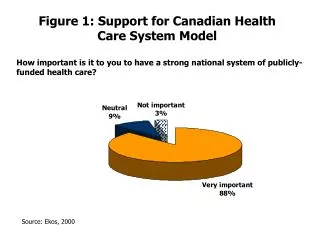
DEMOGRAPHICS OF OEF/OIF VETERANS UTILIZING VA HEALTH CARE • Sex • Male 88% • Female 12% • Age • Under 20 8% • 20 to 29 50% • 30 to 39 22% • Over 40 20% Analysis of Health Care Utilization Among OEF and OIF Veterans
Branch • Air Force 12% • Army 64% • Marine 13% • Navy 12% • Unit Type • Active duty 52% • Reserve/ Guard 48% • Rank • Enlisted 92% • Officer 8%
METHOD OF ACCESS OF SERVICES • Demobilizations • Enrollment Office • OIF/OEF program staff
EXPANSION OF SERVICES • 6000+ OEF/OIF veterans enrolled PVAMC • 3500 ORNG returning from theater April 2010 • Mandated to see veterans within 30 days of enrollment • Mandated to complete TBI secondary within 30 days of positive initial screen
59% of active duty52% of Army Reserves 65% of retired/separated service memberswere exposed to an event or blast that caused a jolt or blow to the head Blast Wave/Blast Wind Report of the President’s Commission on Care for America’s Returning Wounded Warriors – July 30, 2007 (Bob Dole, Donna Shalala – Co-Chairs)
TRAUMATIC BRAIN INJURY: SCREENING OVERVIEW Katherine Noonan, PhD Polytrauma OEF/OIF Psychologist
VA TASK FORCE ON TBI ESTABLISHED DEC 2006 • Addressed need to assess for TBI in returning OEF/OIF (Operation Enduring Freedom/Operation Iraqi Freedom) • Representatives from various fields: • Physical Medicine and Rehabilitation • Neurology • Psychiatry • Psychology • Primary Care • Prevention • Medical Informatics
OUTCOMES OF TASK FORCE • Reviewed • Limited available research on TBI screening • Results from VA’s and Military Treatment Facilities that initiated screening locally • Clinical presentation and natural history of TBI • Consult with Defense and Veterans Brain Injury (DVBIC) • There are currently no validated instruments for TBI screening VHA Directive 2007-013
TBI CLINICAL REMINDER • Screening occurs upon entry into a VA Health Care System • The first step of the reminder is to identify possible Operation Enduring Freedom (OEF)/Operation Iraqi Freedom (OIF) participants based on whether date of separation from military duty or Active Duty status occurred after September 11, 2001. • Screening is done once, for those who confirm OEF/OIF deployment and no prior diagnosis of concussion/mTBI VHA Directive 2007-013
PRIMARY TBI SCREENING-CLINICAL REMINDER • Positive replies in all four sections constitute a positive screen • Events that may increase the risk of TBI • Immediate symptoms following the event • New or worsening symptoms following the event • Current symptoms VHA Directive 2007-013
INITIAL SCREENING IDENTIFIES POSSIBLE TBI • Not all patients with positive initial screen will have TBI • Other diagnoses possible. Examples: • PTSD • Cervico-cranial injury with headache • Positive screens need further evaluation
TBI Secondary Screen • Consultative • Referrals from anywhere in medical center following positive primary screen • Multidisciplinary team approach • Render opinion about cause of symptoms • Close collaboration with other specialties • Case load shared between Post-Deployment Clinic and Polytrauma Clinic
NSI (NeuroBehavioral Symptom Inventory) • Completed during the TBI secondary level evaluations • Outlines common complaints of those individuals who have mTBI and PCS • 22 items-5 point scale • Validated for mTBI • Guides the treatment process
OVERVIEW OF VETERANS SCREENED(PVAMC APRILS 2007-DECEMBER 2009) • 3,911- OIF/OEF veterans screened for possible TBI • 1,022- TBI screen positive (26.1%) • 971- Those who screened positive who agreed to second level evaluation (95%) • 677- Comprehensive Second Level Evaluation Completed (69.7%) • 517- Confirmed TBI diagnosis (76.4%)
POLYTRAUMA SYSTEM OF CARE: OVERVIEW Andrea Karl, MD Polytrauma Program Director
POLYTRAUMA CLINIC “Polytrauma is defined as injury to the brain in addition to other body parts or systems resulting in physical, cognitive and functional disability. Injury to the brain is the impairment which guides the course of rehabilitation.” VHA 2005-24 Directive definition
POLYTRAUMATIC INJURIES Traumatic Brain Injury (TBI) Hearing Loss Amputations Fractures Burns Visual Impairment
POLYTRAUMA REHABILITATION’S ROLE • To care for patients with these diverse and serious injuries requiring more than one type of therapy (physical/occupational/speech) • Interdisciplinary care approach with ongoing follow up
POLYTRAUMA CONTINUUM OF CAREAcute/Trauma Inpatient Outpatient LifetimeCareRehabilitation Rehabilitation Community Care Family Support Case Management Benefits Management
Polytrauma Rehabilitation Centers Polytrauma Network Sites Polytrauma Support Team Clinics Polytrauma Points of Contact GEOGRAPHIC ORGANIZATION
POLYTRAUMA NETWORK SITES • Our closest: VA Puget Sound- Seattle/Tacoma
POLYTRAUMA REHABILITATION CENTERS Tampa Richmond Palo Alto Minneapolis
POLYTRAUMA REHAB CENTERSSCOPE OF CLINICAL SERVICES • Comprehensive Interdisciplinary Inpatient Evaluations • Manage Medical Instability • Acute Comprehensive Inpatient Rehabilitation • Ongoing Follow-up and Care Management Consultation
Specialized interdisciplinary post-acute rehabilitation services; inpatient and outpatient • Manage new patients from inpatient services • Identify local resources for VA and non-VA care • Provide proactive clinical and psychosocial case management; continued support for families • Provide regular follow-up care, check-ups • Coordinate services between VHA, military, private sector
POLYTRAUMA SUPPORT CLINIC TEAMS *Our Site in Portland/Vancouver
POLYTRAUMA SUPPORT CLINIC TEAMS • Outpatient rehabilitation services closer to home- wide distribution across US • Able to care for lifelong impairments with ongoing follow up and family support • Multidisciplinary rehabilitation team approach
POLYTRAUMA POINT OF CONTACT (PPOC) • Point of contact at every VA facility not otherwise designated • Knowledgeable about Polytrauma System of Care • Responsible for Triage and referral to a Polytrauma site
REHABILITATION THERAPIES Occupational Therapy Physical Therapy Speech Therapy
PHYSICAL THERAPIST • Diagnose and treat conditions to restore function and prevent disability • Treat conditions such as head injuries, dizziness, sports injuries, stroke patients, amputees, post-surgical patients, and burn patients among others.
PHYSICAL THERAPISTS EVALUATE: • Sensation • Posture • Coordination • Flexibility • Range of Motion • Strength • Balance • Gait/mobility • Need for braces/prosthesis • Need for assistive devices: • Cane, walker, crutches, wheelchairs
PHYSICAL THERAPY AND TRAUMATIC BRAIN INJURY • Common impairments include: • Dizziness • Poor balance • Other injuries sustained with head injury
OCCUPATIONAL THERAPY Rehabilitative therapy that provides education and training to assist individuals with disabilities to achieve maximal independence in day to day activities that are personally relevant
EXAMPLE AREAS OF INTERVENTION • Activities of daily living (dressing, bathing, hygiene, etc.) • Money mgmt and banking skills • Cooking and kitchen safety • Managing your home • Cognitive planning for daily task • Functional performance • Visual perception • Strength and range of motion
EXAMPLE OF AREAS OF INTERVENTION: • Driving and/or ability to use public transportation • Hand function after injury • Sports after injury
WHO WOULD BENEFIT FROM OT? Individuals with: • Brain Injury • Visually Impaired • Stroke/ CVA • Serious Mental Illness • Hand or upper extremity Injuries • Debilitating Illness (cardiac, respiratory) • Children with developmental disabilities