Download
1 / 27
280 likes | 325 Vues
Explore Albert Ellis's rational-emotive behavior therapy, Beck's cognitive therapy, and their applications in treating psychological conflicts, offering insight into successful cognitive restructuring processes. Learn the key principles and practicalities of cognitive therapies.

E N D
Systems of Psychotherapy:A Transtheoretical Analysis Chapter 10. Cognitive Therapies
A Sketch of Albert Ellis • 1913 - 2007 • First demonstrated rational-emotive therapy (RET) in 1957 • Goal: maximize pleasure & minimize pain • Changed name RET to rational-emotive behavior therapy (REBT) • A charismatic, prolific, & controversial figure
REBT’s Theory of Personality: ABC • Activating (A) events lead to • Beliefs (B) about activating events, which lead to • Emotional Consequences (C) A → B → C
REBT’s Theory of Psychopathology • Psychopathology occurs when irrational beliefs cause emotional consequences • Psychopathology explained by ABC’s A → B → C Not A → C
Main Qualities of Self-Disturbing Philosophies • Beliefs are rigid & dogmatic (e.g., musturbatory thinking) • Beliefs generate unrealistic & over-generalized attributions (e.g., catastrophizing)
REBT’s Therapeutic Processes • Consciousness raising (aware of irrational thinking patterns) • Contingency management (rearrange reinforcements to support behavior changes) • Counterconditioning (replace irrational thinking with rational thinking)
2 Forms of REBT • General or inelegant: synonymous with cognitive-behavior therapy (CBT) • Specialized or elegant: adheres more to Ellis’s formulations
Therapeutic Content Intrapersonal Conflicts • Anxieties & defenses • Self-esteem • Responsibility Interpersonal Conflicts • Intimacy & sexuality • Communication • Hostility • Control
Therapeutic Content (cont.) Indivduo-Social Conflicts • Adjustment versus transcendence • Impulse control Beyond Conflict to Fulfillment • Meaning of life • Ideal individual
Therapeutic Relationship • Seen primarily as precondition for effective treatment • Therapists unconditionally accept client as person, but not necessarily liking or warmth • Therapists evaluate client’s beliefs & behaviors (not as a person) • Self-disclosure is common
Beck’s Cognitive Therapy vs. Ellis’s REBT • Different terminology but similar principles • CT more empiricism than REBT • CT relies more on evidence to alter beliefs while REBT focuses more on philosophical conversion • CT is more structured (e.g., manual adherence, use of checklists), REBT less so • CT is less confrontational than REBT
A Sketch of Aaron Beck • 1921 - • Originally trained in psychoanalytic tradition • Approach heavily rooted in empiricism • Developed popular instruments, including Beck Depression Inventory & Beck Anxiety Inventory • Beck & Ellis did not collaborate but approaches are very similar
CT’s Theory of Psychopathology • Similar to REBT’s theory • Maladaptive cognitions & dysfunctional attitudes cause psychopathology • Underlying cognitions vary specifically with the disorder (cognitive specificity) • Dysfunctional beliefs are not irrational per se, but too absolute, broad, or arbitrary • Schemas: cognitive organization
Several Depressogenic Assumptions • Overgeneralization: one experience applies to all situations • Selective abstraction: only measuring oneself via failure • Excessive responsibility: assuming oneself is responsible for all failures • Self-references: assumption that everyone is paying attention to you, especially at failures • Dichotomous thinking: everything is either one extreme or the other
Cognitive Triad of Depression 1. Events are interpreted negatively 2. Depressed individuals dislike themselves 3. Future is appraised negatively Triad gives rise to maladaptive self-verbalizations or visual images that are experienced as automatic thoughts
Unified Model of Depression • Integrates clinical, cognitive, biological, & evolutionary perspectives • Depression viewed as adaptation loss of essential human resources that access life’s necessities • Model retains cognitive orientation but acknowledges other causal factors
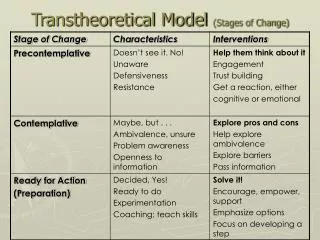
Therapeutic Processes • After symptoms begin to subside (priority number one),tx shifts to underlying cognitions • Identification of problematic schemas & their remediation • Successful clients pass through stages: - Become aware of thinking - Recognize what thoughts are awry - Substitute accurate for inaccurate thoughts
Basic Questions of Cognitive Restructuring • What’s the evidence? • What’s another way of looking at it? • So what if it happens?
Therapeutic Relationship • Collaborative empiricism: shared mission to identify dysfunc thoughts & pursue better ones • Client is an active partner • Therapist provides support & direction; however, empathy is not sufficient • Therapist engenders responsible dependency in client
Practicalities of CT • Time-efficient treatment • 12 – 20 weekly, 50-minute sessions • Sometimesgroup therapy • Treatment is structured by manuals • Bibliotherapy widely used • Homework is expected • Training is widely available
Effectiveness of CT • Hundreds of RCTs conducted • More effective than no treatment & placebo • As or more effective as other treatments for depression, anxiety, panic, PTSD, eating disorders, chronic pain • Not limited to individual therapy (e.g., couple and group cognitive therapy) • CT with homework is more effective than therapy without
Criticisms of Cognitive Therapies • From a Behavioral Perspective (little controlled data, misinterpreted data) • From a Psychoanalytic Perspective (conversion instead of cure) • From a Humanistic Perspective (emphasizes feeling less, negative feelings are not all dysfunctional) • From a Cultural Perspective (lack of consideration for diverse thinking) • From an Integrative Perspective (overgeneralization)
Future Directions • Fastest growing & most researched therapy • Beck is gaining over Ellis • Continued commitment to evaluation, integration, & short-term treatment • Wider application to disabling conditions, e.g., borderline, bipolar, & psychoses • Computer-based CBT interventions on the rise • Schema therapy shows promise for tx of various personality disorders
Key Terms ABC model activating events (A) activity scheduling beliefs (B) catastrophizing cognitive analytic therapy (CAT) cognitive processing therapy (CPT) cognitive restructuring cognitive therapy cognitive triad collaborative empiricism consequences (C) content specificity hypothesis depressogenic assumptions dichotomous thinking disattribution technique disputing/disputation (D) distancing dysfunctional attitudes/cognitions effective new philosophy (E) excessive responsibility hedonism intent-to-treat analysis investigator allegiance
Key Terms (cont.) irrational beliefs (iBs) limited reparenting mindfulness overgeneralization panic control therapy (PCT) PYA—push your ass rational-emotive behavior therapy (REBT) refutations schema focused psychotherapy schemas (cognitive schemas) selective abstraction self-references shame-attacking exercises Socratic dialogue third wave (therapies) tyranny of the should unconditional self-acceptance (USA)
Recommended Websites • Albert Ellis Institute: www.albertellisinstitute.org • Association for Behavioral and Cognitive Therapies: www.abct.org/home • Beck Institute for Cognitive Therapy and Research: www.beckinstitute.org • International Association for Cognitive Psychotherapy: www.the-iacp.com • International Society of Schema Therapy: www.isst-online.com/