Download
1 / 76
830 likes | 1.53k Vues
Pharmacotherapy of antifungal drugs. Isabel Spriet Pharmacy Dpt, UZ Leuven. The fungal ‘players’. Opportunistic fungi Normal flora Candida spp. Ubiquitious in our environment Aspergillus spp. Cryptococcus spp. Mucor spp. Invasive fungal infections - Incidence.

E N D
Pharmacotherapy of antifungal drugs Isabel Spriet Pharmacy Dpt, UZ Leuven
The fungal ‘players’ • Opportunistic fungi • Normal flora • Candida spp. • Ubiquitious in our environment • Aspergillus spp. • Cryptococcus spp. • Mucor spp.
Invasive fungal infections - Incidence • Solid organ transplant: 5-42% • Bone marrow transplant: 15-25% • ICU: 17% Singh N. Clin Infect Dis 2000;31:545-53 Vincent JL. Intens Care Med 1998; 24:206-216
Candidemia – Mortality rate Hospital acquired pathogens and their associated mortality Edmond et al. CID 1999; 29:239-44.
Invasive Aspergillosis – Mortality Rate Review of 1941 Patients from 50 Studies Lin S-J et al, CID 2001; 32:358-66
Fungal infections today A major change in the occurence, diagnosis and management of invasive fungal infections has arisen in the recent years.
Licensed antifungals: a dynamic drug class To be expected: isovuconazole – anidulafungin – micafungin … Posaconazole Voriconazole Caspofungin Lipid amphotericin products Itraconazole Fluconazole Ketoconazole Flucytosine Amphotericin B 1950 1960 1970 1980 1990 2000
OutlineProduct Overview • Spectrum • Therapeutic indications • Recommended dosages • Pharmacokinetics • Pharmacokinetic difficulties and problems • Tolerability and safety • Therapeutic drug monitoring?
An ideal antifungal agent has… • Broad spectrum of activity (yeasts and moulds) • Rapidly and highly fungicidal, stable to resistance • Potent in vivo activity (even in neutropenia) • Good pharmacokinetics (AUC) • Both oral and parenteral formulations • Good penetration into all tissue compartments • Low toxicity, minimal drug-drug interactions • Cost effective
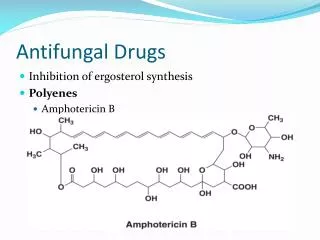
Amphotericin BTarget: fungal cell membrane • Ampho B binds ergosterol in the cell membrane • depolarisation: leakage of monovalent and divalent cations • cell death • stimulates host immune response
Amphotericin BSpectrum and Recommended dosage • Spectrum: • very broad range of activity: most Candida and Aspergillus spp. • active against most fungi except A. terreus, Fusarium spp. • Fungicidal • Amphotericin B: 1 mg/kg IV (after a test dose of 1 mg) • Lipid-based Amphotericin B • amphotericin B Lipid Complex: 5 mg/kg IV • liposomal amphotericin B: 3 mg/kg IV
Amphotericin BPharmacokinetics • Low oral bioavailability: only IV administration • Extensive distribution • High concentrations in liver, spleen, bone marrow • No metabolism • Renal excretion • Halflife: about 5 days
Amphotericin BTolerability and Safety • chills, rigors, fever (during infusion) • nausea, vomiting • cardio/respiratory reactions • phlebitis • can be explained by mode of action: ampho B stimulates host immune response with release of inflammatory cytokines
Amphotericin BTolerability and Safety • Nephrotoxicity: incidence: 49-65% • Hypokalemia can be explained by mode of action: ampho B binds cholesterol in distal tubular membrane leading to wasting of Na+, K+ and Mg++
Amphotericin BTolerability and Safety • Nephrotoxicity has been shown to significantly increase: • Length of hospital stay • Treatment costs • Prevention of nephrotoxicity • Fluids: saline, sodium bicarbonate • Low-dose vasoconstrictors (e.g. dopamine) • Alternate day dosing • Infusion rates (conventional ampho B: at least 6 hrs) • Lipid formulations Bates DW. CID 2001; 32: 686-93. Cagnoni PJ. J Clin Oncol 2000; 18: 2476-83. Greenberg RN. J Med Economics 2002; 2: 109-18.
The azolesTarget: fungal cell membrane • Azoles inhibit ergosterol synthesis by inhibiting 14-α-demethylase • toxic sterol intermediates accumulate in the cell membrane leading to enhanced cellular permeability and inhibition of fungal growth
Inhibits also human CYP450-dependent enzymes playing an important role in human hormone synthesis or drug metabolism DRUG INTERACTIONS!!!
FluconazoleSpectrum, therapeutic indications, dosage • Spectrum: Candida spp. except C. krusei (C. glabrata: reduced susceptibility), Cryptococcus spp. • Indications and dosage: • Prophylaxis in neutropenic patients: fluco 200 mg • Treatment of Candida-infections: Charlier C. JAC 2006; 57:384-410.
FluconazolePharmacokinetics Charlier C. JAC 2006; 57:384-410.
FluconazolePharmacokinetics • Pharmacokinetic problems? • Majority unchanged renal excretion glomerular filtration+ tubular reabsorption • Dose adjustments in severe renal failure • Removed by dialysis: 100 mg extra dose after IHD • Drug interactions: • Inhibits CYP2C9, CYP2C19 and CYP3A4 • cyclosporin – nephrotoxicity: TDM • midazolam: excessive sedation • phenytoin: TDM • tacrolimus – nephrotoxicity, neurotoxicity: TDM • warfarin: INR • Rifampicin induces fluconazole metabolism: • increase fluco dose with 25% Charlier C. JAC 2006; 57:384-410.
FluconazoleTolerability and Safety • Generally very well tolerated: no adverse events • Side effects only occur in high doses (>400 mg/day) • Common: headache, nausea, abdominal pain • Elevated AST/ALT levels: generally mild • Reported in 10% of leukemia patients with fluco prophylaxis • Reported in 20% of ICU patients with fluco prophylaxis • Rare: case reports of fulminant hepatitis • Very rare: • neurotoxicity (high doses > 1200 mg/day), • prolongation of the QT interval Charlier C. JAC 2006; 57:384-410.
FluconazoleTherapeutic drug monitoring? • No routine indications for measuring fluco levels • Predictable fluconazole PK and serum concentrations Charlier C. JAC 2006; 57:384-410.
VoriconazoleSpectrum of activity • Invasive aspergillosis • fungicidal activity as great as ampho B • Invasive candidiasis • C. glabrata? • Fusarium, Penicillium, Scedosporium • Cryptococcus • in vitro activity > flucytosine or fluconazole • ! Zygomycetes: resistant to voriconazole • Breakthrough infections Mashmeyer G et al. Future Microbiol 2006; 1: 365-85.
VoriconazoleRecommended dosage • Loading dose: 2 x 6mg/kg • Maintenance dose: 2 x 4 mg/kg • Infusion over 1hr • Adult Patients < 40 kg • Loading dose idem • Maintenance dose: 2 x 2 mg/kg or 2 x 100 mg • Child A and B cirrhosis (Child C: no data) • Loading dose idem • Maintenance dose: 2 x 2 mg/kg or 2 x 100 mg • Children (2-12 yrs) • 2 x 7 mg/kg
VoriconazolePharmacokinetics Voriconazole serum levels: high interindividual variability! !Difficult pharmacokinetics! • Non-linear kinetics: saturable metabolism! • Disproportional increase in plasma levels if dosage increased • Half-life = dose dependent • In children: linear pharmacokinetics: higher metabolising capacity • Dosage 7 mg/kg bid • Genetic polymorphism CYP2C19 • 3 genotypes: extensive metabolizers, heterozygous extensive metabolizers, poor metabolizers • PM especially in Asian population: 18-23% • PM in Caucasion population: 3-5% • Plasma levels up to 2-fold (HEM) or 4- fold (PM) higher! Purkins L et al. AAC 2002; 46:2546-53.
VoriconazolePharmacokinetics • Extensive CYP-metabolism: drug interactions! • Other drugs affecting voriconazole plasma levels • Contra-indicated with potent inducers • Rifampicin, ritonavir, carbamazepine, phenobarbital • Dose adjustments needed if combined with phenytoin (5 mg/kg bid) • Voriconazole affecting plasma levels of others (inhibition) • Contra-indicated with sirolimus, terfenadines, astemizole, cisapride, … • Dose adjustments needed if combined with • Cyclosporin (- 50% ): if not, risk of nephrotoxicity • Tacrolimus (- 66%): if not, risk of nephrotoxicity
VoriconazolePharmacokinetics • Oral bio-availability affected if taken with food • reduction oral bio-availability with > 20%! • no studies if administered with enteral feeding on ICU • Stop enteral feeding 1hr before up to 2 hrs after administration • Administration 2x daily: 6 hrs without calory intake! Purkins L et al. Br J Clin Pharmacol 2003; 56 (S1): 17-23
VoriconazoleSafety • Visual disturbances: (20%) • Altered perception of light, photophobia, blurred vision, color vision changes: mechanism unknown • transient, infusion related • more in patients with higher levels - how to assess in sedated patients? • Hepatotoxicity (13%) • AST, ALT, alkaline phosphatase, bilirubin elevations • AST, ALP and BILI abnormalities correlating with higher vorico plasma levels • Phototoxicity (6%): erythema, Steven-Johnson syndrome, toxic epidermal necrolysis • Neurological changes: confusion and hallucinations
VoriconazoleSafety • Adverse effects of voriconazole • French pharmacovigilance database • 4 year registration period • detailed registration of cases • causality assessment • Results • LFT abnormalities in 23% patients • Visual disturbances in 18% of patients • Skin rashes in 17% of patients • Cardiovascular events (10%), hematologic disorders (8%) renal disturbances (4%) Eiden C. Ann Pharmacother 2007; 41:755-63
VoriconazoleTolerability and Safety • Nephrotoxicity of SBECD • IV vials contain SBECD, a solubilizer • in patients with moderate to severe renal failure (CrCl < 50 ml/min): accumulation of SBECD with potential nephrotoxicity (vacuolization of urinary epithelium) • frequent problem in ICU patients: switch to oral formulation? Or other product? Von Mach MA et al. BMC Clin Pharamacol 2006; 6:6
VoriconazoleTherapeutic drug monitoring? • Complex pharmacokinetics High inter and intra- individual variability!! • Serum levels correlated with efficacy/safety? • Optimal serum levels: 2-6 µg/ml • Well above MIC of Aspergillus/Candida spp.
VoriconazoleTherapeutic drug monitoring? • TDM voriconazole • 52 adult patients: 181 samples • 25%: levels < 1mg/L • Correlated with oral therapy • Lack of response more frequent in this group • 31%: levels > 5.5 mg/L • Correlated with omeprazole comedication • 5 patients with neurotoxicity • 4 of 5 treated intravenously • TDM improves efficacy and safety • Proposed therapeutic interval 1-5.5 µg/ml • Pascual A. CID 2008;46:201-211.
VoriconazoleTherapeutic drug monitoring? • TDM … • in all patients? • in patients with progressive disease? • in patients exhibiting significant visual or hepatic toxicity? • in patients at risk of fluctuating plasma levels? • drug interactions? • changing hepatic and renal function? • treated by mouth? • ICU? • daily (cost-effectiveness)? • method? • dose adjustments? • non-lineair kinetics! Goodwin M et al. JAC 2007. Epub
PosaconazoleSpectrum, therapeutic indication and dosage • Spectrum: Candida spp. (less active C. glabrata), Aspergillus spp., C. neoformans, H. capsulatum, Zygomycetes • Indications: • Prophylaxis of invasive fungal infections in high-risk patients (SCTx – GvHD, AML-MDS) • Treatment of IA, fusariosis, chromoblastosis, mycetoma, coccidiomycosis refractory to ampho B or itra • Dosage: 200 mg 3 - 4x/day • Only available as oral suspension
PosaconazolePharmacokinetics Schiller D et al. Clin Ther 2007; 29: 1862-1886
PosaconazolePharmacokinetics Posaconazole levels: high interindividual variability! !Difficult pharmacokinetics! • Absorption • 2.6-4-fold higher if taken with a meal • High-fat meals enhance absorption • Cimetidine: gastric pH: 40% decrease in posaconazole AUC and Cmax • Avoid concomitant use of histamine 2-blockers or PPIs! • Mucositis? Schiller D et al. Clin Ther 2007; 29: 1862-1886 Goodwin M et al. JAC 2007. Epub.
PosaconazolePharmacokinetics • Drug interactions • Posaconazole inhibits CYP3A4 (not a substrate of CYP3A4) • Tacrolimus: dose reduction with 66% • Cyclosporine: dose reduction with 25% • Increase in serum concentrations of benzodiazepines, calcium channel blockers, statines, TCA, nevirapine… • Posaconazole is substrate of UGT 1A4 • Induction by phenytoin: contra-indicated! • Induction by rifabutin: contra-indicated! Schiller D et al. Clin Ther 2007; 29: 1862-1886 Goodwin M et al. JAC 2007. Epub.
PosaconazolePharmacokinetics • Dosing in patients with hepatic impairment? • posaconazole should be used with caution • not studied using Child score • Dosing in patients with renal impairment? • Dose adjustment not necessary • Use with caution in severe renal failure Schiller D et al. Clin Ther 2007; 29: 1862-1886 Goodwin M et al. JAC 2007. Epub.
Posaconazole Tolerability and Safety • Gastro-intestinal side effects • Abdominal pain, diarrhea, vomiting: 3-7% • Elevated liver function tests • Rash - Not correlated with elevated posa serum levels Schiller D et al. Clin Ther 2007; 29: 1862-1886 Goodwin M et al. JAC 2007. Epub.
PosaconazoleTherapeutic drug monitoring? • Limited data available • FDA approved product information: • association between posa levels and efficacy • Proven (6%) or probable (3.8%) IFI if levels < 0.7 µg/ml • Proven (1.8%) or probable (0%) IFI if levels > 0.7 µg/ml lower concentrations correlate with treatment failure • recommendations: • ensurance of adequate plasma levels: • Administration of posaconazole with a meal • Avoidance of drug inducing agents • Monitoring for breakthrough infections Goodwin M et al. JAC 2007. Epub.
PosaconazoleTherapeutic drug monitoring? • TDM in patients with: • Progressive disease • Suspected poor oral absorption (nausea, vomiting, mucositis, compliance) • Levels > 1.25 mg/L Goodwin M et al. JAC 2007. Epub.
The echinocandinsTarget: fungal cell wall • Echinocandines inhibit 1,3-beta-glucan synthase • depletion of glucan polymers: weak cell wall