Download
1 / 36
470 likes | 2.25k Vues
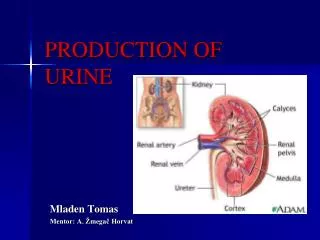
Renal mechanisms of diluting and concentrating urine. Renal mechanisms of diluting and concentrating urine. The kidneys excrete excess water by forming dilute urine and conserves water by excreting concentrated urine. Can excrete urine with an osmolarity as low as 50mOsm/L

E N D
Renal mechanisms of diluting and concentrating urine concentration&dilution of urine
Renal mechanisms of diluting and concentrating urine • The kidneys excrete excess water • by forming dilute urine • and conserves water by excreting concentrated urine. • Can excrete urine • with an osmolarity as low as 50mOsm/L • Conversely, can excrete urine • with concentration of 1200 –1400mOsm/L. concentration&dilution of urine
Renal mechanisms of diluting and concentrating urine • ADH alters renal excretion of water • independent of rate of solute excretion. • ADH secretion when the solute • in the body fluids become too concentrated. • It increases the permeability • of late distal tubules and collecting ducts to water. concentration&dilution of urine
Excretion of dilute urine • When there is a large excess of water in the body • the kidneys can excrete as much as 20L/day of dilute urine. • Continue to reabsorb solutes • while failing to reabsorb large amount of water in distal parts of the nephron. • Glomerular filtrate has osmolarity that of plasma. concentration&dilution of urine
Excretion of dilute urine • In proximal tubules, • solutes and water are reabsorbed • in equal proportions, so that • little change in osmolarity occur. concentration&dilution of urine
Excretion of dilute urine • In the descending loop of Henle • water is reabsorbed by osmosis • and the tubular fluid reaches equilibrium • with surrounding interstitial fluid. concentration&dilution of urine
Excretion of dilute urine • Ascending limb of loop of Henle • is impermeable to water • even in presence of large amounts of ADH. concentration&dilution of urine
Excretion of dilute urine • Active reabsorption of solutes, • causing the tubular fluid to become more dilute • as it flows into the early distal tubule, • osmolarity decreasing • progressively to 100mOsm/L. concentration&dilution of urine
Excretion of dilute urine • In the distal tubules, cortical collecting duct and medullary duct • there is additional reabsorption of NaCl. • In the absence of ADH • these segments are also impermeable to water. concentration&dilution of urine
Excretion of dilute urine • Tubular fluid become even more dilute • decreasing its osmolarity • to as low • as 50 mOsm/L concentration&dilution of urine
Excretion of concentrated urine • Essential for survival of mammals • that live on land. • Fluid intake is required • to match with fluid loss. • The ability of the kidney • to form a small volume of concentrated urine • minimizes the intake required to maintain homeostasis. concentration&dilution of urine
Excretion of concentration urine • When there is water deficit in the body • the kidney forms small volume concentrated urine • by continuing to excrete solutes • while increasing water reabsorption. • Obligatory urine volume 0.5l/day. • Excretion of concentrated urine requires. • High ADH level. • Hyperosmotic renal medullary interstitium. concentration&dilution of urine
Excretion of concentrated urine H2O NaCl H2O NaCl Urea 300 100 300 300 cortex NaCl 600 600 600 600 H2O NaCl H2O medullar NaCl 1200 1200 1200 1200 Urea concentration&dilution of urine
Stimuli for ADH secretion • ECF osmolarity • Blood volume/Arterial pressure • Stimuli to CNS • Drugs, • Alcohol inhibits ADH secretion concentration&dilution of urine
Hyperosmotic renal medullary interstitium • Provide osmotic gradient • necessary for water reabsorption to occur • in the presence of high levels of ADH • Water moves • through the tubular membrane by osmosis • into the renal interstitium • then by vasa recta back into the blood. concentration&dilution of urine
Causes of hyperosmotic renal medullary interstitium • Special anatomical arrangements • of the loops of Henle and vasa recta. concentration&dilution of urine
Causes of hyperosmotic renal medullary interstitium • Major factors that contribute to hyperosmolarity • of renal medullary interstitium are • Active transport of Na+, and cotransport of K+, Cl- • and others out of the thick portion of loop of Henle. • Capable of establishing concentration gradient • of 200 mOsm/L • Active transport of ions • from the collecting duct into the medullary interstitium. • Passive diffusion of urea • from inner medullary collecting ducts into the interstitiusm concentration&dilution of urine
Causes of hyperosmotic renal medullary interstitium • Diffusion of only small amount of water • from the medullary collecting ducts • into the medullary interstitium. • large amount being reabsorbed • in late distal tubules and cortical collecting ducts. • Some passive reabsorption of NaCl • in the descending loop of Henle. concentration&dilution of urine
Mechanisms • Active pump • of thick ascending limb of loop of Henle • establishes 200mOsm/L concentration gradient • between the tubular fluid and interstitial fluid. concentration&dilution of urine
Mechanisms • Tubular fluid in the descending limb • of loop of Henle and the interstitial fluid • quickly reach osmotic equilibrium. • Hyperosmotic fluid • formed in the descending limb • flows into ascending limb. concentration&dilution of urine
Mechanisms • Once this fluid • is in the thick segment • additional ions • are pumped into the interstitium • with water remaining behind • until osmotic gradient of 200mOm/L • is established. concentration&dilution of urine
Mechanisms • Tubular fluid in the descending loop • and hyperosmotic medullary interstitial fluid • reaches equilibrium. concentration&dilution of urine
Mechanisms • These are repeated • over and over with the net effect • of adding more and more solutes to the medulla in excess of water. concentration&dilution of urine
Mechanisms • With sufficient time • this process multiplies • the concentration gradient • established by active transport of ions • in the thick segment of loop of Henle • raising the osmolarity • to 1200 – 1400mOm/L • This process • Counter current multiplier. concentration&dilution of urine
Mechanisms • Passive reabsorption of urea • from inner medullary collecting ducts • contributes 40% of the renal medullary interstitium osmolarity • when the kidney is forming maximally concentrated urine. concentration&dilution of urine
Mechanisms • Very little urea • is reabsorbed in the loop of Henle. • Distal tubules and cortical collecting ducts • are impermeable to urea • even in the presence of high concentration of ADH. concentration&dilution of urine
Mechanisms • In the presence of high [ADH], • Urea] increases rapidly in cortical collecting duct. concentration&dilution of urine
Mechanisms • As fluid flows • into inner medullary collecting ducts • further reabsorption • of water takes place, • [Urea] increase. concentration&dilution of urine
Mechanisms • Increased [Urea] • causes large amount of urea • to diffuse into the interstitium • because this segment • is highly permeable to urea • ADH increases • this permeability even more. concentration&dilution of urine
Urea cycle • Urea is recycled • several times before it is excreted. • Some diffusion of urea • into the thin loop of Henle from the medullary interstitium. concentration&dilution of urine
Maintenance of hyperosmolarity of the renal medulla • Medullary blood flow is low • The vasa recta serves as counter current exchangers, • Minimizing wash out of solutes from the medullary interstitium. • Blood enters and leaves the medulla by the way of vasa recta at the boundary of cortex and medulla. concentration&dilution of urine
Maintenance of hyperosmolarity of the renal medulla • As blood descends into the medulla • toward the papillae • it becomes progressively more concentrated • party by solute • entry from the interstitium concentration&dilution of urine
Maintenance of hyperosmolarity of the renal medulla • and party by water diffusing • into the interstitium • By the time • blood reaches the tips of vasa recta • it has conc. of 1200mOm/L. concentration&dilution of urine
Maintenance of hyperosmolarity of renal medulla • As blood ascends back • toward the cortex • it become progressively less concentrated • water moving into vasa recta • solutes diffusing out. concentration&dilution of urine
Maintenance of hyperosmolarity of renal medulla • Thus although there is • large amount of fluid and solute exchange • across the vasa recta, • there is little • net dilution of the concentration • of the interstitial fluid at each level of the medulla. concentration&dilution of urine
Renal medullary Vasa recta mOsm/L Renal medullary interstitium interstitium 300 300 300 solutes solutes H2O 600 600 600 solutes 600 solutes H2O 800 800 900 solutes 800 solutes H2O 1000 1200 1200 concentration&dilution of urine