Download

1 / 136
1.39k likes | 1.55k Vues
Explore classes of anticoagulant drugs that prevent coagulation, dissolve clots, and prevent bleeding and hemorrhage. Learn about the different drug classes, prototypes, actions, effects, and complications associated with anticoagulants. Discover how anticoagulants target factors to prevent thromboembolism, with a focus on drugs like Heparin, Warfarin, and more. Understand the mechanism of action, complications, and treatment of Heparin-induced thrombocytopenia.

E N D
Classes of Drugs Prevent coagulation Dissolve clots Prevent bleeding and hemorrhage - Hemostatic Overcome clotting deficiencies (replacement therapies)
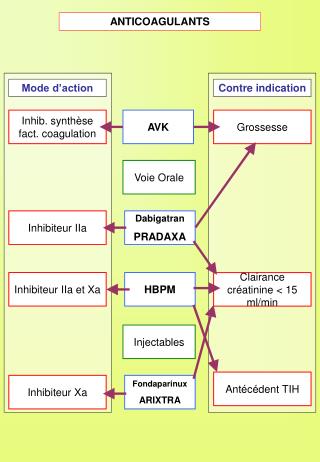
Anticoagulant drugs to treat thromboembolism Drug Class Prototype Action Effect Anticoagulant Parenteral Inactivation of clotting Factors Heparin Prevent venous Thrombosis Anticoagulant Oral Warfarin Decrease synthesis of Clotting factors Prevent venous Thrombosis Prevent arterial Thrombosis Antiplatelet drugs Aspirin Decrease platelet aggregation Breakdown of thrombi Thrombolytic Drugs Streptokinase Fibinolysis
Heparin Sulphated carbohydrate Different sizebovine lungs Administration - parenteral- Do not inject IM - only IV or deep s.c. Half-life 1 - 5 hrs - monitor aPTT Adverse effect: hemorrhage Antidote : protamine sulphate
DRUG TARGETS Unfractionated heparin(UFH)
DRUG TARGETS LOW MOLECULAR WEIGHT HEPARIN(LMWH) Enoxaparin
Heparin mechanism of action Heparin Antithrombin III Thrombin
Complications of Heparin Haemorrhage Heparin-induced thrombocytopaenia (HIT) Osteoporosis (long-term only)
Heparin-Induced Thrombocytopaenia Most significant adverse effect of heparin after haemorrhage Most common drug-induced thrombocytopenia A large number of patients receive heparin in the hospital environment.
Non-immune heparin-associated thrombocytopaenia (“HIT Type I”) Benign Up to 10% patients on heparin Rapid decline in platelet count within first 2 days of heparin administration Platelet count >100 000/ul Returns to normal within 5 days despite continued heparin use (or within 2 days if heparin is stopped).
Heparin-induced thrombocytopaenia: “HIT type 2” Potentially catastrophic thrombosis (Heparin-induced thrombocytopenia and thrombosis) 8% of patients on heparin develop antibody without becoming thrombocytopenic 1-5% patients on heparin develop thrombocytopaenia Of those with thrombocytopaenia, 30% develop venous and/or arterial thrombosis Bleeding uncommon
Treatment of HIT Discontinue all heparin If need to continue anti-coagulation, use danaparoid (orgaran). Avoid platelet transfusions Thrombosis: use danaparoid or thrombin inhibitor
Oral anticoagulants Examples: Coumarins - warfarin, dicumarol Structurally related to vitamin K Inhibits production of active clotting factors Clearance is slow - 36 hrs Delayed onset 8 - 12 hrs Overdose - reversed by vitamin K infusion Can cross placenta - do not use during late pregnancies
Mechanism of action Descarboxy Prothrombin Prothrombin Reduced Vitamin K Oxidized Vitamin K NAD NADH Warfarin Normally, vitamin K is converted to vitamin K epoxide in the liver. →This epoxide is then reduced by the enzyme epoxide reductase. →The reduced form of vitamin K epoxide is necessary for the synthesis of many coagulation factors (II, VII, IX and X, as well as protein C and protein S). →Warfarin inhibits the enzyme epoxide reductase in the liver, thereby inhibiting coagulation. (عبدالله المطيري)
Antiplatelet drugs Example: Aspirin Prevents platelet aggregation /adhesion Clinical use - prevents arterial thrombus Myocardial infarction (MI), stroke, heart valve replacement and shunts Other antiplatelet drugs are - Dipyridamole, sulfinpyrazone and Ticlopidine
Mechanism of action Aspirin inhibits cyclooxygenase (COX) COX is a key enzyme involved in the synthesis of thromboxane 2 (prostaglandins) Inhibits platelet aggregation
Prophylactic use of Aspirin Low dose daily. Prevents ischemic attack (ministroke) and MI 335 mg/day reduced the risk of heart attack in patients over 50 More than 1000 mg/day NO EFFECT Contraindication - DO NOT give to patients with glucose 6-PO4 dehydrogenasedeficiency
Definition of Anticoagulation Therapeutic interference ("blood-thinning") with the clotting mechanism of the blood to prevent or treat thrombosis and embolism.
Indications of Anticoagulant Therapy Treatment and Prevention of Deep Venous Thrombosis Pulmonary Emboli Prevention of stroke in patients with atrial fibrillation, artificial heart valves, cardiac thrombus. Ischaemic heart disease During procedures such as cardiac catheterisation and apheresis.
Hemostasis requires a fine balance between procoagulant and regulatory factors Coagulation Proteins/ Platelets/ Vessel wall PC PS ATIII… Thrombosis Deficiency Deficiency/ Abnormality Bleeding
Thrombosis - Pathogenesis 3 primary influences predispose to thrombus formation Virchow’s Triad (1856): Endothelial Injury Stasis Hypercoagulability
Clinical significance of thrombosis Obstruction of arteries and veins Ischemia or necrosis of downstream tissue Embolization
Deep vein thrombosis (DVT) and acute pulmonary embolism (PE) are two manifestations of venous thromboembolism (VTE). VTE contributes to significant morbidity and mortality both in the community and in hospital. The mainstay of therapy for DVT is anticoagulation, provided there is no contraindication. Following initial anticoagulation, patients with DVT are anticoagulated further to prevent future recurrences, embolism, and thrombosis-related death.
Initial anticoagulation is administered in the first 5 to 10 days following a diagnosis of DVT. Long-term anticoagulant therapy is typically administered for a finite time beyond the initial period, usually three to six months, and occasionally up to 12 months. Extended anticoagulation refers to therapy that is administered indefinitely.
Anticoagulation is the mainstay of therapy for patients with deep venous thrombosis (DVT). Anticoagulation is indicated for all patients with proximal deep venous thrombosis (DVT) and select cases of distal DVT. The decision to anticoagulate must weigh the benefits of anticoagulation against the risk of bleeding for an individual.
The primary objective of anticoagulation is the prevention of further thrombosis and of early and late complications. Major early complications of DVT include further clot extension, acute pulmonary embolus (PE), major bleeding, and death. Late complications include recurrent clot, post-thrombotic (post phlebitic) syndrome and chronic thromboembolic pulmonary hypertension.
Duration of therapy — A decision regarding the optimal duration of anticoagulation must take into account the presence or absence of provoking events, risk factors for recurrence and bleeding, as well as to the individual patient's preferences and values. Although there is agreement on the minimum length of time a patient with a first episode of DVT should be treated (ie, three months), the optimal length of time is not known. For most patients with a first episode of proximal DVT (provoked and unprovoked, proximal and distal), anticoagulants should be administered for three months rather than for shorter periods (eg, four or six weeks) (algorithm 1).
Algorithm for the treatment of lower extremity deep venous thrombosis (DVT) - a first episode of DVT.
Most experts agree that extending anticoagulation beyond three months is considered in select populations, particularly in patients with provoked DVT with persistent but reversible risk factors (extended finite periods; eg, 6 to 12 months or until risk factor is resolved) and unprovoked DVT (indefinite anticoagulation). In contrast, anticoagulation beyond three months is NOT typically performed in patients with an episode of DVT provoked by a transient risk factor (eg, surgery) or in those at high risk of bleeding.
Pregnancy — Pregnancy is a risk factor for the development of DVT. Adjusted-dose subcutaneous LMW heparin is the preferred agent for initial and long-term anticoagulation in pregnant women with acute DVT. This agent is preferred, because it has a more favorable safety profile, especially when compared with warfarin. Warfarin freely crosses the placental barrier and can produce an embryopathy when given between the sixth and ninth weeks of pregnancy. Intravenous and subcutaneous forms of unfractionated heparin are alternatives to LMW heparin. Fondaparinux and oral factor Xa and direct thrombin inhibitors have not been adequately tested in pregnant women with acute DVT and as such should not be administered.
The optimal duration of anticoagulation in pregnancy is unknown and should be individualized on a case-by-case basis. In general, the total duration of anticoagulant therapy (pregnancy plus the postpartum period) should be at least three to six months for women whose only risk factors for DVT were transient (eg, pregnancy, cesarean section). Anticoagulant therapy generally continues for at least six weeks postpartum. Patients with persistent risk factors for DVT may require a longer duration of therapy.
Arterial Thrombosis Most common cause of death in Western industrialized countries Myocardial infarction due to thrombotic occlusion of a coronary artery is the #1 cause of death Endothelial damage Atherosclerosis Hypertension Hypercholesterolemia Radiation Endotoxins (in bacterial infection)
Venous Thrombi Most occur in the superficial or deep veins of the leg (DVT) Superficial thrombi Swelling and pain Rarely embolize DVT Pain, redness and swelling Asymptomatic in 50%
Pathophysiology of Pulmonary Embolism Tapson V. N Engl J Med 2008;358:1037-1052
Warfarin Mechanism of Action II VII IX X Synthesis of Non Functional Coagulation Factors Antagonism of Vitamin K
Antithrombotic Agents: Mechanism of Action Anticoagulants: prevent clot formation and extension Antiplatelet drugs: interfere with platelet activity Thrombolytic agents: dissolve existing thrombi
Warfarin: Indications Prophylaxis and/or treatment of: Venous thrombosis and its extension Pulmonary embolism Thromboembolic complications associated with AF and cardiac valve replacement Post MI, to reduce the risk of death, recurrent MI, and thromboembolic events such as stroke or systemic embolization Prevention and treatment of cardiac embolism
Warfarin: Major Adverse Effect - Hemorrhage Factors that may influence bleeding risk: Intensity of anticoagulation Concomitant clinical disorders Concomitant use of other medications Quality of management
High risk categories: Any patient with the following must be considered as a high risk of bleeding when on warfarin and the reversal of warfarin may be considered at a lower INR. • Age >65 • Uncontrolled hypertension • Diabetes • Renal failure • Hepatic failure • Trauma and recent surgery • Anti platelet drugs • Previous major bleeding
Special Considerations in the Elderly—Bleeding Increased age associated with increased sensitivity at usual doses Comorbidity Increased drug interactions ? Increased bleeding risk independent of the above
Prothrombin Time (PT) Historically, a most reliable and “relied upon” clinical test However: Proliferation of thromboplastin reagents with widely varying sensitivities to reduced levels of vitamin K-dependent clotting factors has occurred Concept of correct “intensity” of anticoagulant therapy has changed significantly (low intensity) Problem addressed by use of INR (International Normalized Ratio)
INR: International Normalized Ratio A mathematical “correction” (of the PT ratio) for differences in the sensitivity of thromboplastin reagents Relies upon “reference” thromboplastins with known sensitivity to antithrombotic effects of oral anticoagulants INR is the PT ratio one would have obtained if the “reference” thromboplastin had been used Allows for comparison of results between labs and standardizes reporting of the prothrombin time
INR Equation INR = International Normalized Ratio ISI = International Sensitivity Index
Potential Problems with the INR Limitations Unreliable during induction Loss of accuracy with high ISI thromboplastins Incorrect ISI assignment by manufacturer Incorrect calculation of INR due to failure to use proper mean normal plasma value to derive PT ratio Solutions Use thromboplastin reagents with low ISI values (less than 1.5) Use thromboplastin reagents with low ISI values Use thromboplastin reagents with low ISI values and use plasma calibrants with certified INR values Use “mean normal” PT derived from normal plasma samples for every new batch of thromboplastin reagent
Warfarin: Dosing Information Individualize dose according to patient response(as indicated by INR) Use of large loading dose not recommended May increase hemorrhagic complications Does not offer more rapid protection Low initiation doses are recommended for elderly/frail/liver-diseased/malnourished patients
Conversion from Heparin to Warfarin May begin concomitantly with heparin therapy Heparin should be continued for a minimum of four days Time to peak antithrombotic effect of warfarin is delayed 96 hours (despite INR) When INR reaches desired therapeutic range, discontinue heparin (after a minimum of four days)