Download
1 / 10
120 likes | 468 Vues
Peritoneal Dialysis for Elderly Patients: A Review. Source: Tesar V. Peritoneal dialysis in the elderly—is its underutilization justified? Nephrol Dial Transplant. 2010;1– 4. Overview.

E N D
Peritoneal Dialysis for Elderly Patients: A Review Source: Tesar V. Peritoneal dialysis in the elderly—is its underutilization justified? Nephrol Dial Transplant. 2010;1– 4.
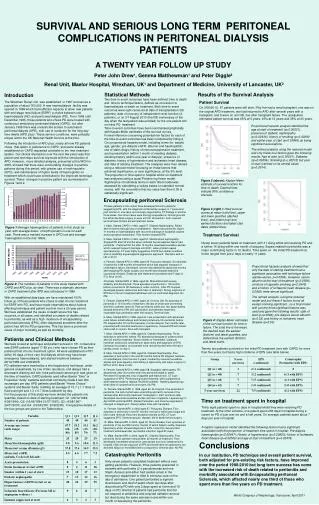
Overview • Peritoneal dialysis (PD) is an underused dialysis process followed in the elderly population due to inadequate data on PD outcomes and quality-of-life (QOL) as compared to other dialysis options. • Peritoneal dialysis is used in <15% of patients with end-stage renal disease, but it has a vast disparity at the international and regional levels. • Several studies have shown that the outcomes with PD and hemodialysis (HD) are alike, and patients subjected to PD first may even demonstrate better clinical results. • However, there are trials which have revealed that PD is associated with a higher mortality rate, when the modality is started from the second year of treatment. • These studies also have suggested that there are potential survival benefits if the dialysis process is timely switched off from PD to HD. • In the UK, incident dialysis patients in the age group of more than 65 years are twice less likely to be on PD in comparison with younger patients.
Broadening Options for Long-Term Dialysis in the Elderly Study • This cross-sectional study analyzed the various aspects of QOL like cognitive function, index of deprivation and illness intrusiveness in matched patients of more than 65 years of age, across the PD and HD methods. Study Design • Dialysis patients (at least 90 days on dialysis) but not hospitalized for at least 30 days were included in the study. • Apart from assessing the occurrence and severity of 16 symptoms commonly seen among older people and patients on dialysis, the Illness Intrusiveness Ratings Scale was employed to evaluate the effect of kidney disease and dialysis modality related to 13 dissimilar domains of life.
Findings • The The Broadening Options for Long-term Dialysis in the Elderly (BOLDE) study successfully and adequately matched HD and PD patients across several vital variables, apart from comorbidity scores, which were greater in HD patients. • The high comorbidity scores showed a direct effect on the short form-12 (SF-12) mental component score in malnourished patients and augmented the possibility of clinical depression. However, there was no impact on the illness intrusion or SF-12 physical component. • The QOL parameters were influenced by the symptom count significantly.
Findings • The observations are as follows: • Although there were no vital variations in patient characteristics among the PD and HD patients, racial minorities and significantly female patients were less expected to take part as a PD patient in the study. • The HD and PD patients did not vary in the unadjusted QOL and physical component scores. • The PD patients had slightly but extensively improved mental component scores, lesser number of symptoms and significantly fewer possible depression and lower illness intrusion. • Differences in the mental component were observed only in patients who underwent dialysis for >12 months. • Possible depression (hospital anxiety and depression scale >8) was much superior in female patients and this amplified with each additional symptom and comorbidity. • Illness intrusion was apparently superior in young patients and those with more symptoms. In addition, illness intrusion was also independently linked with dialysis. • There was no difference in the PD and HD patients related to cognitive function, nutrition or social network.
Findings • Some other studies that have dealt with older patients receiving dialysis include north thames dialysis study, which showed no variation in results or QOL among HD and PD patients. • The netherlands cooperative study of the adequacy of dialysis (NECOSAD) study demonstrated that when patients are appropriately educated and an option to choose dialysis modality is given then approximately 50% select PD. • About 6–19% of patients in the BOLDE study were treated by PD as compared to 27% of patients in the NECOSAD study in patients ranging from 65 to 70 years and compared with 19% of patients in the 70 years age group.
Conclusion • The QOL is similar in the PD and HD patients. • The BOLDE and Nephrology Dialysis Transplantation studies, however have shown that PD offers better QOL as compared to HD. • The PD modality should be encouraged in the older population. • The availability of adequate and proper data about PD also has an important role to play in its success in elderly patients with end-stage kidney disease, who are supposed to be ineligible for the dialysis modality due to comorbidities, cognitive and sensory dysfunction and social exclusion.
Conclusion • Findings from the European Renal Best Practice Advisory Board indicated that preferences for HD may be counteracted by a better education of predialysis patients who are given the chance to choose between PD and HD. • In addition, limitations like reduced representation of women and ethnic minorities, bias in selecting the HD population and a comparatively low number of studied patients, which limited the possibility of subgroup analyses (e.g., diabetics and nondiabetics) should be looked into.
Conclusion • Social contraindications, which contribute to 40% of the overall PD contraindications, can be partly reduced through proper training of nurses. • Although it is not possible to educate patients with later referral (frequently treated with HD), such late referral does not entirely exclude PD. All patients (including the older group) should be given an equivalent right to similar care services and opportunities to select the dialysis method, which should not be influenced by any slight cost differences or on the local nephrologist’s motivation.