Download
1 / 49
640 likes | 1.47k Vues
Antipsychotic Therapy: Managing Extrapyramidal Effects. John Lauriello , M.D. Extrapyramidal Side Effects of Antipsychotic Medications. Parkinsonism and Dystonia Tardive Dyskinesia Akathisia Neuroleptic Malignant Syndrome. Effectiveness of a Particular Treatment.

E N D
Antipsychotic Therapy: Managing Extrapyramidal Effects John Lauriello, M.D.
Extrapyramidal Side Effects of Antipsychotic Medications • Parkinsonism and Dystonia • Tardive Dyskinesia • Akathisia • Neuroleptic Malignant Syndrome
Effectiveness of a Particular Treatment • Extent to which a particular treatment helps individuals afflicted with a particular illness in their lives • = Efficacy + Tolerability + Compliance
Rule#1: Efficacy FirstSide Effects SecondRule #2: No Side EffectNo Effect
Tolerability • Nuisance (patient comfort) vs life threatening • Often time-limited • Often easily managed • Mild-moderate EPS, prolactin elevation, sexual dysfunction Side Effects of AntipsychoticsTolerability vs Safety • Mixed Safety & Tolerability • Akathisia • Weight gain • Metabolic risk factors • Sedation • Safety • Life threatening • Acute or chronic • Cardiovascular disease, metabolic syndrome, diabetes • NMS, laryngospasm Adapted from Newcomer, JW. J Clin Psychiatry. 2007;68(suppl1):20-27.
Barriers to Medication Adherence in Schizophrenia Stigma Adverse drug reactions Homelessness / substance abuse Forgetfulness Lack of social support Afraid of medication Denial of illness Lack of trust in provider Difficulty with regimen Patients (n=153 ) reporting barriers (%) Hudson et al 2004 J Clin Psychitatry
Rank Order of Side Effects Eliciting Moderate-to-Severe Distress Patients Reporting Moderate-to-Severe Distress (N=99) 50 40.0 37.3 40 33.2 30.8 30 Percent 18.8 18.4 20 10 0 Akathisia(N=38) Akinesia(N=49) WeightGain(N=58) Anticho- linergic(N=45) SexualProblems (N=39) MuscleRigidity(N=32) Weiden PJ, Miller AL (2001), J Psychiatr Pract 7(1):41-47
Treatment Discontinuation in CATIE :Owing to Intolerability Mean modal dose Ziprasidone 112.8 mg/day Risperidone 3.9 mg/day Quetiapine 543.4 mg/day Olanzapine 20.1 mg/day Perphenazine 20.8 mg/day n=183 Ziprasidone 15 n=333 Risperidone 10 n=329 Quetiapine 15 n=330 Olanzapine 19 n=257 Perphenazine 16 0 10 20 30 40 50 Patients (%) Lieberman JA et al. N Engl J Med. 2005;353:1209-1223.
Patient Discontinuations in CATIE Weight or metabolic effects EPS Sedation OLZ QTP PER RIS ZIP *P=.001 vs other agents. Lieberman JA et al. N Engl J Med. 2005;353:1209-1223.
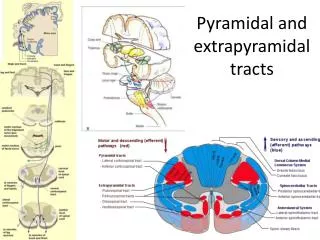
Prefrontal DA Terminal Lesion Normal State PrefrontalCortex Prefrontal Cortex Limbic Sites Limbic Sites Brain StemDA Neurons Brain StemDA Neurons Modified DA Hypothesis of Schizophrenia Pycock et al, 1981; Davis et al, 1991; Weinberger DR. Arch Gen Psychiatry. 1987;44:660
Disruption of Dopamine Pathways Leads to Predictable Effects Mesocortical Pathway Disruption Nigrostriatal Pathway Disruption • Negative symptoms • Cognitive impairment • Depression • Dystonia • Akinesia • Rigidity • Tremor • Dyskinesia Hypothalamic Disruption • Prolactin elevation • Amenorrhea • Galactorrhea • Sexual dysfunction • Mesolimbic Pathway Disruption • Agitation, psychosis, mania, disorganization, thrill/drug seeking Inoue A, Nakata Y (2001), Jpn J Pharmacol 86:376-380; Seesack SR, Carr DB (2002), Physiol Behavior 77:513-517
D2 Occupancy Predicts Response 100 80 Responders 60 Nonresponders % Responders (CGI) 40 20 0 <60 >65 Striatal D2 Occupancy (%) D2 occupancy predicts response on CGI (p<0.001); Predicts change in positive symptoms PANSS (p=0.07); Kapur S et al. (2000), Am J Psychiatry 157(4):514-520
D2 Occupancy Predicts EPS/Akathisia 78% D2 Occupancy (%) Individual Participants • No participant <78% showed EPS/akathisia Kapur S et al. (2000), Am J Psychiatry 157(4):514-520
Χ Signs of Motor EPSBegin Schematic of D2 Occupancy, Antipsychotic Efficacy and EPS Liability 100 80 60 % Receptor Occupancy 40 20 0 Dose
Dosing and Relative EPS Vulnerability Schematic Diagram of Dose and Relative EPS Liability 100 Haloperidol Risperidone Likelihood of EPS (%) 50 Ziprasidone Olanzapine Quetiapine 0 Low Moderate High Very High Therapeutic Dosing Jibson MD, Tandon R (1998), J Psychiatr Res 32(3-4):215-228
D2 Receptor Partial Agonist High D2 Affinity With Low D2 Side Effects Aripiprazole Risperidone Olanzapine Quetiapine Haloperidol Ziprasidone Clozapine D2 0.34* 0.7 4 5 11 125 160 *Aripiprazole has high D2 affinity but not high D2 antagonism! Data represented as Ki (nM); Bymaster FP et al. (1996), Neuropsychopharmacology 14(2):87-96; Seeger TF et al. (1995), J Pharmacol Exp Ther 275(1):101-113; Daniel DG et al. (1999), Neuropsychopharmacology 20(5):491-505; Arnt J, Skarsfeldt T (1998), Neuropsychopharmacology 18(2):63-101
D2 receptor Full activation Full agonist (dopamine) No activation Antagonist (haloperidol, etc.) Partial activation Partial agonist (aripiprazole) Aripiprazole: The Exception An Agonist Has Intrinsic Activity: Ability of a Compound to Activate Receptors
(Antipsychotic) AEs (EPS) AEs (EPS) 0.3 1 3 10 30 Dose (mg/kg) Antipsychotics Atypical Typical 100 100 (Antipsychotic) 75 75 Effect 50 50 Effect 25 25 0 0 0.3 1 3 10 30 Dose (mg/kg) Casey DE. Motor & Mental Aspects of EPS. Int Clin Psychopharmacol. 1995(Sept);10(suppl 3):105-114
Atypical Antipsychotics for Schizophrenia TMAP Schizophrenia Clinician’s Manual. http://www.dshs.state.tx.us/mhprograms/pdf/SchizophreniaManual_060608.pdf. Accessed October 2010. FDA. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.Search_Drug_Name. Accessed October 2010.
Barriers to EPS Diagnosis • Outdated notion that EPS is a therapeutic benefit • Difficulty getting accurate history • Acceptance of EPS as part of mental illness • Overlap between behavioral manifestations of EPS and psychiatric symptoms • Lack of training in EPS diagnosis • Belief that atypical antipsychotics do not cause EPS
Advantages of EPS Sparing Antipsychotics NegativeSymptomBenefit Lower Riskof TD LessNoncompliance CognitiveAdvantage Fewer EPS Fewer MotorSide Effects Less Dysphoria Tandon R et al. (1999), J Clin Psychiatry 60 Suppl 8:21-28
Frequency of Antipsychotic-Induced Parkinsonism (Conventional Antipsychotics) Parkinson Type Incidence (%) Any 61 Akinesia 33 Rigidity 52 Tremor 23 Weiden P (1994), In: DSM-IV Sourcebook, vol. 1. Washington, D.C.: American Psychiatric Publishing, Inc.
Parkinsonism Rates of Aripiprazole vs. Haloperidol (Simpson-Angus Scale) 1.4 1.2 1 0.8 0.6 S-A Score Change From Baseline 0.4 0.2 0 -0.2 -0.4 -0.6 Placebo 2 mg Ari 10 mg Ari 15 mg Ari 20 mg Ari 30 mg Ari 10 mg Hal N= 40 58 161 195 194 245 183 *p0.01; Marder SR et al. (2003), Schizophr Res 61(2-3):123-136
Parkinsonism Rates: Quetiapine vs. Haloperidol (Simpson-Angus Scale) 50 40 * 30 Percent of Patients Placebo Quetiapine Hal 20 10 0 75 150 300 600 750 12 Dose (mg/day) *p<0.05 vs. placebo; Arvanitis L, Miller BG (1997), Biol Psychiatry 42(4):233-246
The Risk of Tardive Dyskinesia Is Not Trivial 5-Year Prospective Incidence in Elderly with Conventional Antipsychotics Mean Rx length: 114.7 weeks Average dose: 80 mg/day CPZ equivalent Mean age: 76.9 yrs 1-year incidence: 25% N = 261 100 80 Cumulative Percent 95% CI 60 % of Patients with TD 40 20 0 0 26 52 78 104 130 156 182 208 234 260 Weeks Patient population included dementia, major mood disorders, schizophrenia/schizoaffective disorder, anxiety disorders Woerner MG, et al. Am J Psychiatry. 1998;155(11):1521-1528.
Risperidone TD: 1-Year Prospective Incidence in the Elderly 14 Median Rx length: 273 days Mean modal dose: 0.96 mg/day Mean age: 82.5 years 1-year incidence: 2.6% N = 330 12 10 8 % of Patients with TD 6 4 2 0 0 30 60 90 120 150 180 210 240 270 300 330 365 Days of Treatment Jeste DV, et al. Am J Psychiatry. 2000;157:1150-1155.
Mean Weighted 1-Year Incidence Rates of Tardive Dyskinesia 6.8 7 5.4 6 5.3 5 Mean Rate of TardiveDyskinesia (%) 4 3 2 0.8 0.41 1 0 Children (N=783, 10 Trials) Adults (N=1,964, 6 Trials*) Adults and Elderly(N-207, 1 Trial) Elderly (N=521, 4 Trials*) Haloperidol-Treated Adults(N=408, 3 Trials) Participants Treated With SGAs *1 study reported separate rates for tardive dyskinesia in adults and the elderly Correll CU et al. (2004), Am J Psychiatry 161(3):414-425; 1Correll CU, Kane J (in press), J Child Adolesc Psychopharmacol
Incidence of TD with Second-Generation Antipsychotics in 1-Year Studies Mean Age (Years) Mean Dose (mg/Day) Exposure (Days) Annualized TD Incidence (%) Author Drug N Glazer, 1999 Quetiapine 301 36 475 272 (mean) 0.74* Rein, 1999 Amisulpride 331 36 624 359 (median) 1.5 Haloperidol 106 39 14.6 352 (median) 5.9 Beasley, 1999 Olanzapine 513 37 13.5 260 (median) 0.52* Haloperidol 114 36 13.9 259 (median) 7.4* Sanger, 2001 Olanzapine 97 39 13.9 198 (mean) 0 Csernansky, 2002 Risperidone 177 40 4.9 364 (median) 0.6 Haloperidol 188 40 11.7 238 (median) 4.1 Chouinard, 2002 Risperidone 587 42 55.2 350 (median) 0.71 Microspheres Arato, 2002 Ziprasidone 207 50 92.0 206 (median) 6.8 Placebo 71 49 - 72 (median) 35.7 Davidson, 2000 Risperidone 139 73 3.7 Not reported 13.4* Jeste, 1999 Quetiapine 85 76 172 365 (median) 2.72* Jeste, 2000 Risperidone 255 82 0.96 273 (median) 2.6* Correll CU, Leucht S, Kane JM: Am J Psychiatry 2004 ; 161:414-425
Olanzapine vs. Haloperidol TD: 1-Year Prospective Incidence 14 Haloperidol 1-year incidence: 7.45% N=114 Olanzapine 1-year incidence: 0.52% N=513 p=0.002 olanzapine vs. haloperidol 12 10 8 % of Patients with TD 6 4 2 0 0 42 100 200 300 400 500 600 700 Days of Treatment Beasley et al. Randomized, double-blind comparison of the incidence of tardive dyskinesia in patients with schizophrenia during long-term treatment with olanzapine or haloperidol. Br J Psychiatry. 1999(Jan);174:23-30
Akathisia Subjective Sense of Restlessness Objective Sense of Restlessness Associated Distress Often described as coming from the body Associated with medication use Is it really an EPS?
Causes of Restless Syndromes(Akathisia differential) Idiopathic Antipsychotics Antidepressants Anti-emetics: Metoclopromide, Prochloperazine, Promethazine Stimulants: Amphetamines, Caffeine, Coffee Antihistamines Drug Withdrawal: Opiates, Barbiturates, Cocaine, Benzodiazepines. Alcohol, Cannabis Serotonin Syndrome Chondromalacia patella
When Akathisia Is Missed Akathisia Akathisia not diagnosed Raise in dose worsens akathisia Doctor responds to worsening of “psychosis” Dose “Psychosis”
Neuroleptic Malignant Syndrome NMS life-threatening (10%) complication of treatment with antipsychoticdrugs Fever, severe muscle rigidity,and autonomic and mental status changes Estimatesof the incidence once ran as high as 3% of patients treatedwith antipsychotics, more recent data suggest an incidence of0.01%–0.02% Reintroduction of antipsychotics possible Strawn et al Am J Psychiatry 164:870-876, June 2007
Neuroleptic Malignant Syndrome F – Fever A – Autonomic instability L – Leukocytosis T – Tremor E – Elevated enzymes (elevated CPK) R – Rigidity of muscles
NMS-Differential Encephalitis Status Epilepticus Heat Stroke Malignant Hyperthermia Serotonin Syndrome Drug Intoxication
PORT Psychopharmacology Treatment Recommendations • Evidence for differences among antipsychotic agents in the risk for developing EPS ranking is high-potency FGAs > mid-potency FGAs = risperidone > low-potency FGAs > olanzapine, ziprasidone > quetiapine > clozapine. • There is currently insufficient evidence to rank aripiprazole nor to further refine the ranking of FGAs. • FGA medications, prophylactic use of antiparkinson agents to reduce the incidence of EPS should be determined on a case by case basis. The use of prophylactic antiparkinson agents in people treated with SGA medications is not warranted. • SGA medications, including clozapine, and several adjunctive agents have been evaluated for the treatment of TD. However, there is insufficient evidence to support a recommendation for the use of any specific agent to treat TD. • NMS occurs rarely but has been associated with treatment with both FGA and SGA medications. Since the last update, there is additional evidence available on the risk of NMS with antipsychotic medications, including clozapine, and therefore, the previous recommendation to select clozapine as the first-line treatment for individuals with previous NMS is no longer being included. There is insufficient evidence to recommend the use of a specific antipsychotic medication for people who have previously developed NMS. Buchanan et al Schizophrenia Bulletin 2010 Jan, 36 (1) 71-93
Reduce Dopamine Blocking Load EPS appears to be dose related Use lowest maintenance oral dose Consider switching to long acting antipsychotic agent Switch to a different antipsychotic Use an “antidote” medication
* * * * Olanzapine Risperidone All Conventional Low-Dose Monotherapy Monotherapy Monotherapy Haloperidol (N=60) (N=49) (N=161) (N=38) Switching to Quetiapine: Degree of EPS Reduction as a Function of Prior Antipsychotic -35 -30 Improvement -25 -20 -15 -10 -5 0 Previous Antipsychotic ITT population; *p<0.001 vs. baseline; †Mean PANSS total score baseline value; LSM = least square mean; LVCF = last value carried forward; De Nayer A et al. (2002), Poster presented at the 23rd Annual Meeting of the CINP, Montreal, Canada: June 23-27
Agents for Treating Tardive Dyskinesia May be reversible but not guaranteed No proven medication treatment Agents that increase dopamine blockade temporarily help--”vicious cycle” Studies of Vitamin D, Omega 3 fatty acids have not held up to large scale studies
Agents for Treating NMS Benzodiazepines Amantadine 200-400 mg/day Bromocriptine 7.5mg-45 mg/day Dantrolene sodium 1-2.5mg IV initially and then 1mg q6hrs with eventual switch to oral ECT
Achieving Best Outcomes with Antipsychotics • EFFECT FIRST! • Minimize impairment by side-effects • NO EPS • NO USE OF ANTICHOLINERGIC • MINIMIZE OTHER ADVERSE EFFECTS • INDIVIDUALIZE THERAPY • MONITOR ON AN ONGOING BASIS • AND THEN MAKE NECESSARY ADJUSTMENTS