Download
1 / 17
170 likes | 286 Vues
Long Stay Patient Project “Stranded Patients”. 08 April 2013 Presented by Andrew Davies Project Leaders: Alicia Sutton, Charlotte Porter. ADHB %<6 Hour Performance. The Problem: Not just in ED. Why Focus on Long Stay Patients?. Voice of staff

E N D
Long Stay Patient Project “Stranded Patients” 08 April 2013 Presented by Andrew Davies Project Leaders: Alicia Sutton, Charlotte Porter
Why Focus on Long Stay Patients? • Voice of staff • Recommended next steps from other acute flow projects (e.g. Daily Rapid Rounds) • Literature Review • Healthcare Advisory Board – Maximizing Hospital Capacity (2002)
ADHB General Medicine – Evaluating the Opportunity Patients with Over 10 Day Length of Stay LOS > 10 Days LOS > 10 Days Patients with Over 21 Day Length of Stay LOS > 21 Days LOS > 21 Days ADHB General Medicine Discharges from July 2004 to March 2013
The Project • Initiated Long-Stay Patient Project in General Medicine – April 2012 • Clinical note review conducted of all > 21 day patients discharged from December 2010 to December 2011 • Implemented first improvements from July 2012 to December 2012 • Leveraged results and actions to other service areas
Causes for Delay - Over 21 Day Patients Top Causes • Rest Home / Private Hospital Placement • PPPR • Social Work Input • Older Peoples Health Review & Placement
Other Observations During Audit • Significant variation in practice of how the plan for the stay is managed • No standard Admission to Discharge process followed for 1st time Rest Home / Private Hospital patients • No escalation criteria to involve Service Manager, Nurse Advisor & Clinical Director. • Poor visibility of current long-stay patients leading to variation in management
Increase Visibility in Service of Long Stay Patients • Daily Long Stay Patient report automated, reviewed by Nurse Specialists & Charge Nurses (July – 2012)
Increase Visibility in Service of Long Stay Patients • Long Stay Patient Report reviewed and discussed weekly at General Medicine Production Meeting (October 2012) • Issues escalated to Service Manager, Nurse Advisor & Clinical Director • Charge Nurses, Nurse Specialists & Nurse Educators also attend
Increase Visibility in Service of Long Stay Patients • Include LOS on Patient Status at a Glance whiteboards on Wards 65, 66, 67, 68 (January 2013) • Visible in Nursing Station and can be flagged at Daily Rapid Rounds Current LOS Added to Whiteboards
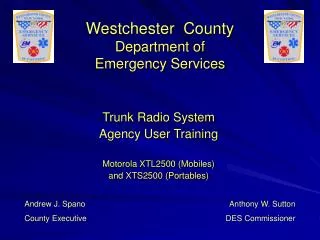
Results: Proportion of Over 10 Day LOS Patients Lowest Proportion of > 10 Day Patients Ever @ 6.1% (January to March 2013) • Daily Rapid Rounds implemented (Feb 2010) • New medical model of care implemented (Dec 2011) • Split Acute (APU) & Inpatient Ward • 4-8 p.m. on-call consultant on-site • Additional weekend medical staff • Long Stay Project Commenced (Apr 2012) • Long Stay Patient Visibility and Standard Escalation Practices implemented (Sep-Dec 2012) Quarterly Proportion of > 10 Day LOS Patients since July 2007 Key Projects 1 3 4 2 1 2 3 4
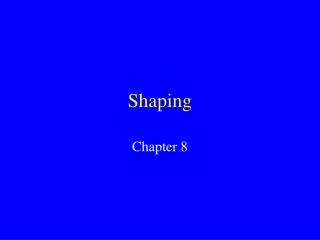
Results: General Medicine Average Length of Stay Shortest Quarterly Average Length of Stay Ever @ 2.97 (January to March 2013) • Daily Rapid Rounds implemented (Feb 2010) • New medical model of care implemented (Dec 2011) • Split Acute (APU) & Inpatient Ward • 4-8 p.m. on-call consultant on-site • Additional weekend medical staff • Long Stay Project Commenced (Apr 2012) • Long Stay Patient Visibility and Standard Escalation Practices implemented (Sep-Dec 2012) Quarterly Average LOS Patients since July 2004 Key Projects 1 3 4 2 1 2 3 4
Results: General Medicine Average Length of Stay Quarterly Average LOS Patients since July 2004 4 2 1 0.5 day reduction in Average LOS ~ 6,000 bed days/yr
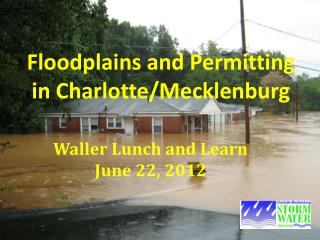
What Next - We need to focus on the whole system with initiatives on each part of the journey Community (Home) Other DHBs / Private Provider Community (Home) Hospice 5 15 16 7 19 15 DCCM ED Medical 9 2 18 12 Follow-up Clinic 11 20 GP APU Radiology WARD 18 REHAB 9 17 18 CLINIC Surgical Operating Rooms 3 6 8 13 3 4 7 7 Residential Care Residential Care 1 4 Patient Transit Supply Chain Labs Pharmacy Therapies 14 IMTS 11 10 Hospital Ops 15 Demand Management Flow Improvement
Initiatives to reduce acute demand to secondary facilities Community (Home) Other DHBs / Private Provider Community (Home) Hospice Avoidable presentations from ARRC Reduce the % of St John transports for status 3 and 4 patients Use of the GAIHN predictive risk algorithm Cluster model for ARRC Gen Med Acute clinics Advance Care plan (Implementation) Acute clinic pathways Reducing Readmissions 5 7 DCCM ED Medical 9 2 Follow-up Clinic GP APU Radiology WARD REHAB 9 CLINIC Surgical Operating Rooms 3 6 8 3 4 7 7 Residential Care Residential Care 1 4 Patient Transit Supply Chain Labs Pharmacy Therapies IMTS Hospital Ops 16 Demand Management
Initiatives to improve the flow within secondary facilities 10. Integrated Ops centre 11. Management of escalation practices 12. Improved utilization of bed capacity at GSU 13. Elimination of duplicated documentation between AED and IP specialties 14. National shared care plan 15. Matching medical resources to demand 16. Coordination between AED and IP 17. Stranded Patients 18. Proactive discharging 19. Medical HDU and enhanced DCCM admission criteria 20. Ward based flow improvement initiatives Community (Home) Other DHBs / Private Provider Community (Home) Hospice 15 16 19 15 DCCM ED Medical 18 12 Follow-up Clinic 11 20 GP APU Radiology WARD 18 REHAB 17 18 CLINIC Surgical Operating Rooms 13 Residential Care Residential Care Patient Transit Supply Chain Labs Pharmacy Therapies 14 IMTS 11 10 Hospital Ops 17 Flow Improvement