Download
1 / 96
990 likes | 1.17k Vues
Ethics Influenza vaccines Healthcare workers. Johan Bester ( MBChB , Mphil Applied Ethics) Department of Family Medicine, University of Calgary. Is there a shift?. Many hospitals and states in the US have mandatory policies. Is there a shift?.

E N D
EthicsInfluenza vaccines Healthcare workers Johan Bester (MBChB, Mphil Applied Ethics) Department of Family Medicine, University of Calgary
Is there a shift? • Many hospitals and states in the US have mandatory policies
Is there a shift? • Many hospitals and states in the US have mandatory policies • Los Angeles County
Los Angeles County • “Every healthcare worker in an acute care hospital, nursing facility or intermediate care facility to either receive the influenza vaccination annually, or wear a mask during flu season when in contact with patients.”
British Columbia • Recently passed similar requirement
Pushback • Not accepted by all staff
Pushback • Not accepted by all staff • This differs from other required vaccinations – MMR, Hep B
Objectives • Ethical basis for such requirements
Objectives • Ethical basis for such requirements – THUS: • The usual ethical argument for these requirements
Objectives • Ethical basis for such requirements – THUS: • The usual ethical argument for these requirements • Analyze the argument in light of current evidence
Objectives • Ethical basis for such requirements – THUS: • The usual ethical argument for these requirements • Analyze the argument in light of current evidence • Conclude whether argument is successful
Objectives • Ethical basis for such requirements – THUS: • The usual ethical argument for these requirements • Analyze the argument in light of current evidence • Conclude whether argument is successful • Implications
Caplan’s argument • Professional duty to place patients first, vaccination benefits patients Caplan AL. Morality of influenza Vaccine Mandates. Clinical Therapeutics Volume 35, Number 2, 2013
Caplan’s argument • Professional duty to place patients first, vaccination benefits patients • Duty to do no harm, vaccination prevents harm Caplan AL. Morality of influenza Vaccine Mandates. Clinical Therapeutics Volume 35, Number 2, 2013
Caplan’s argument • Professional duty to place patients first, vaccination benefits patients • Duty to do no harm, vaccination prevents harm • Protect the vulnerable, vaccination prevents spread to the vulnerable Caplan AL. Morality of influenza Vaccine Mandates. Clinical Therapeutics Volume 35, Number 2, 2013
Caplan’s argument • Professional duty to place patients first, vaccination benefits patients • Duty to do no harm, vaccination prevents harm • Protect the vulnerable, vaccination prevents spread to the vulnerable • Obligation to set an example for the public Caplan AL. Morality of influenza Vaccine Mandates. Clinical Therapeutics Volume 35, Number 2, 2013
Caplan’s argument • Professional duty to place patients first, vaccination benefits patients • Duty to do no harm, vaccination prevents harm • Protect the vulnerable, vaccination prevents spread to the vulnerable • Obligation to set an example for the public • Voluntary measures failed to ensure adequate vaccination Caplan AL. Morality of influenza Vaccine Mandates. Clinical Therapeutics Volume 35, Number 2, 2013
Caplan’s argument • Professional duty to place patients first, vaccination benefits patients • Duty to do no harm, vaccination prevents harm • Protect the vulnerable, vaccination prevents spread to the vulnerable • Obligation to set an example for the public • Voluntary measures failed to ensure adequate vaccination • Mandatory vaccination policies increase vacc rates Caplan AL. Morality of influenza Vaccine Mandates. Clinical Therapeutics Volume 35, Number 2, 2013
Caplan’s argument • Professional duty to place patients first, vaccination benefits patients • Duty to do no harm, vaccination prevents harm • Protect the vulnerable, vaccination prevents spread to the vulnerable • Obligation to set an example for the public • Voluntary measures failed to ensure adequate vaccination • Mandatory vaccination policies increase vacc rates THUS: Ethical to have a mandatory vaccination policy Caplan AL. Morality of influenza Vaccine Mandates. Clinical Therapeutics Volume 35, Number 2, 2013
Zimmerman’s argument • Vaccinating HCW benefits patients, prevents harm, and has low risk of harm Zimmerman RK. Ethical analyses of institutional measures to increase health care worker influenza vaccination rates. Vaccine 31 (2013) 6172-6176
Zimmerman’s argument • Vaccinating HCW benefits patients, prevents harm, and has low risk of harm • Beneficence and non-maleficence trump personal autonomy for HCW in this case Zimmerman RK. Ethical analyses of institutional measures to increase health care worker influenza vaccination rates. Vaccine 31 (2013) 6172-6176
Zimmerman’s argument • Vaccinating HCW benefits patients, prevents harm, and has low risk of harm • Beneficence and non-maleficence trump personal autonomy for HCW in this case • Best way to prevent harm is vaccinating HCW; other measures may not be feasible (eg work absence or neg press ventilation) Zimmerman RK. Ethical analyses of institutional measures to increase health care worker influenza vaccination rates. Vaccine 31 (2013) 6172-6176
Zimmerman’s argument • Vaccinating HCW benefits patients, prevents harm, and has low risk of harm • Beneficence and non-maleficence trump personal autonomy for HCW in this case • Best way to prevent harm is vaccinating HCW; other measures may not be feasible (eg work absence or neg press ventilation) • Mandatory programs with infect control measures for non-compliance ensures best vaccination coverage Zimmerman RK. Ethical analyses of institutional measures to increase health care worker influenza vaccination rates. Vaccine 31 (2013) 6172-6176
Zimmerman’s argument • Vaccinating HCW benefits patients, prevents harm, and has low risk of harm • Beneficence and non-maleficence trump personal autonomy for HCW in this case • Best way to prevent harm is vaccinating HCW; other measures may not be feasible (eg work absence or neg press ventilation) • Mandatory programs with infect control measures for non-compliance ensures best vaccination coverage • This also provides a way to opt-out for those with objections – wear a mask the whole flu season Zimmerman RK. Ethical analyses of institutional measures to increase health care worker influenza vaccination rates. Vaccine 31 (2013) 6172-6176
The Argument • Significant illness/burden of disease
The Argument • Significant illness/burden of disease • HCW vaccination prevents spread to patients
The Argument • Significant illness/burden of disease • HCW vaccination prevents spread to patients • High rate HCW vaccination lowers M&M in patients
The Argument • Significant illness/burden of disease • HCW vaccination prevents spread to patients • High rate HCW vaccination lowers M&M in patients • Voluntary programs – low rate HCW vaccination
The Argument • Significant illness/burden of disease • HCW vaccination prevents spread to patients • High rate HCW vaccination lowers M&M in patients • Voluntary programs – low rate HCW vaccination • Duty to benefit and to do no harm
The Argument • Significant illness/burden of disease • HCW vaccination prevents spread to patients • High rate HCW vaccination lowers M&M in patients • Voluntary programs – low rate HCW vaccination • Duty to benefit and to do no harm • Professional duty limits HCW autonomy/rights
The Argument • Significant illness/burden of disease • HCW vaccination prevents spread to patients • High rate HCW vaccination lowers M&M in patients • Voluntary programs – low rate HCW vaccination • Duty to benefit and to do no harm • Professional duty limits HCW autonomy/rights Thus: Justified to impose program of mandated Influenza vaccination on HCW Opt-out: wear a mask during flu season
An Argument: • Premise 1 • Premise 2 Conclusion: Follows from premise 1 and 2
An Argument: • Premise 1 • Premise 2 Conclusion: Follows from premise 1 and 2 Examining an argument: Are the premises true? Is the logic sound?
Important premises in The Argument • Influenza is an important public health problem with significant mortality and morbidity
Important premises in The Argument • Influenza is an important public health problem with significant mortality and morbidity • Vaccination is very successful in limiting spread and impact
Important premises in The Argument • Influenza is an important public health problem with significant mortality and morbidity • Vaccination is very successful in limiting spread and impact • Vaccinating HCW provides protection to patients
Important premises in The Argument • Influenza is an important public health problem with significant mortality and morbidity • Vaccination is very successful in limiting spread and impact • Vaccinating HCW provides protection to patients • Vaccination has an acceptable risk of harm
Important premises in The Argument • Influenza is an important public health problem with significant mortality and morbidity • Vaccination is very successful in limiting spread and impact • Vaccinating HCW provides protection to patients • Vaccination has an acceptable risk of harm • Masks are effective (preventing spread in unvaccinated)
Influenza is important • Seems to be true; does seem to have significant M&M
Influenza is important • Seems to be true; does seem to have significant M&M • Exact burden of disease not known
Influenza is important • Seems to be true; does seem to have significant M&M • Exact burden of disease not known • Part of larger problem “Influenza-like-illness”
Influenza is important • Seems to be true; does seem to have significant M&M • Exact burden of disease not known • Part of larger problem “Influenza-like-illness” • Don’t routinely test those with ILI for influenza
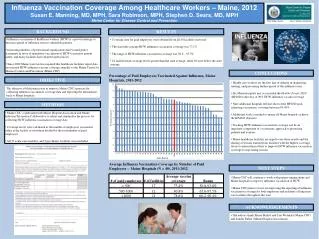
Influenza is important • Seems to be true; does seem to have significant M&M • Exact burden of disease not known • Part of larger problem “Influenza-like-illness” • Don’t routinely test those with ILI for influenza • Pub Health Canada reported 3,450 hospitalizations and 189 deaths in their report 2-8 March 2014
Influenza is important • Seems to be true; does seem to have significant M&M • Exact burden of disease not known • Part of larger problem “Influenza-like-illness” • Don’t routinely test those with ILI for influenza • Pub Health Canada reported 3,450 hospitalizations and 189 deaths in their report 2-8 March 2014 • Mathematical models say 2000-8000 deaths each year
Influenza is important • Seems to be true; does seem to have significant M&M • Exact burden of disease not known • Part of larger problem “Influenza-like-illness” • Don’t routinely test those with ILI for influenza • Pub Health Canada reported 3,450 hospitalizations and 189 deaths in their report 2-8 March 2014 • Mathematical models say 2000-8000 deaths each year • May be more, may be less.
Influenza is important • Can accept this, with proviso – morbidity and mortality not exactly known
Vaccine is very effective • “Vaccine is very successful in limiting the spread and impact of influenza.”
Vaccine is very effective • Bad year = 44% effective (95% CI 23% to 59%) • Good year = 73% effective (95% CI 54% to 84%) Jefferson T et al. Vaccines for preventing influenza in healthy adults (Review). Cochrane Database of Systematic Reviews, Issue 6, 2013
Vaccine is very effective • Bad year = 44% effective (95% CI 23% to 59%) • Good year = 73% effective (95% CI 54% to 84%) • Results of review: Influenza vaccination had modest effect in time off work and limiting influenza duration. Jefferson T et al. Vaccines for preventing influenza in healthy adults (Review). Cochrane Database of Systematic Reviews, Issue 6, 2013
Vaccine is very effective • Bad year = 44% effective (95% CI 23% to 59%) • Good year = 73% effective (95% CI 54% to 84%) • Results of review: Influenza vaccination had modest effect in time off work and limiting influenza duration. • No evidence for reducing complications of ILI or transmission Jefferson T et al. Vaccines for preventing influenza in healthy adults (Review). Cochrane Database of Systematic Reviews, Issue 6, 2013