
Evaluation of Caucasian and Multi-Ethnic Spirometry Prediction Equations in Tunisian Adults
This study investigates the applicability of Caucasian and multi-ethnic spirometric prediction equations in interpreting spirometry data among Tunisian adults. A total of 38 subjects, including healthy non-smokers and smokers, were evaluated using the Tunisian reference equations, ECCS1983, and GLI2012. Results showed significant discrepancies when applying Caucasian or multi-ethnic equations, suggesting potential misinterpretation of lung function data. This highlights the necessity for tailored reference values in the Tunisian population for accurate spirometric assessment.

Evaluation of Caucasian and Multi-Ethnic Spirometry Prediction Equations in Tunisian Adults
E N D
Presentation Transcript
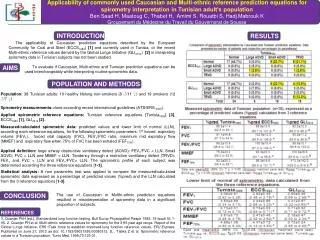
Applicability of commonly used Caucasian and Multi‐ethnic reference prediction equations for spirometry interpretation in Tunisian adult’s population Ben Saad H, Maatoug C, Thabet H, Amimi S, Rouatbi S, Hadj Mabrouk K Groupement du Médecine du Travail du Gouvernorat de Sousse INTRODUCTION AIMS POPULATION AND METHODS CONCLUSION RESULTS The applicability of Caucasian prediction equations described by the European Community for Coal and Steel (ECCS1983) [1] and currently used in Tunisia, or the recent Multi‐ethnic reference values derived by the Global Lungs Initiative (GLI2012) [2] in interpreting spirometry data in Tunisian subjects has not been studied. To evaluate if Caucasian, Multi-ethnic and Tunisian prediction equations can be used interchangeably while interpreting routine spirometric data. Population: 38 Tunisian adults: 19 healthy lifelong non-smokers (8 ♂/11 ♀) and 19 smokers (12 ♂/7 ♀) Spirometry measurements: done according recent international guidelines (ATS/ERS 2005). Applied spirometric reference equations: Tunisian reference equations [Tunisia1995] [3], ECCS1983[1], GLI2012 [2]. Measured/calculated spirometric data: predicted values and lower limit of normal (LLN), according each reference equations, for the following spirometric parameters: 1st forced expiratory volume (FEV1), forced vital capacity (FVC), FEV1/FVC ratio, maximum mid expiratory flow (MMEF) and expiratory flow when 75% of FVC has been exhaled (FEF75%). Applied definition: large airway obstructive ventilatory defect (AOVD): FEV1/FVC < LLN. Small AOVD: FVC > LLN and MMEF < LLN. Tendency through a restrictive ventilatory defect (TRVD): FEV1 and FVC < LLN and FEV1/FVC> LLN. The spirometric profile of each subject was determined according the three reference equations [1-3]. Statistical analysis: A non parametric test was applied to compare the measured/calculated spirometric data expressed as a percentage of predicted values (%pred) and the LLN calculated from the 3 reference equations [1-3]. The use of Caucasian or Multhi-ethnic prediction equations resulted in misinterpretation of spirometry data in a significant proportion of subjects. REFERENCES 1. Quanjer PhH (ed.). Standardized lung function testing. Bull Europ Physiopathol Respir 1983; 19 (supll 5): 1-95. 2. Quanjer PH et al. Multi-ethnic reference values for spirometry for the 3-95 year age range. Report of the Global Lungs Initiative, ERS tTask force to establish improved lung function reference values. ERJ Express. Published on June 27, 2012 as doi: 10.1183/09031936.00080312. 3. . Tabka Z et al. Spirometric reference values in a Tunisian population. Tunis Med. 1995;73:125-31.





