Download

1 / 66
891 likes | 2.69k Vues
Pathophysiology of Acute & Chronic Pain. Steven Stanos, DO Center for Pain Management Rehabilitation Institute of Chicago Dept. of PM&R, Northwestern University Medical School Feinberg School of Medicine. Nociceptive vs. Neuropathic Receptors and channels Inflammation

E N D
Pathophysiology of Acute & Chronic Pain Steven Stanos, DO Center for Pain Management Rehabilitation Institute of Chicago Dept. of PM&R, Northwestern University Medical School Feinberg School of Medicine
Nociceptive vs. Neuropathic • Receptors and channels • Inflammation • Peripheral Sensitization • Central Sensitization • Temperature Sensation • Plasticity & Brain Changes • Muscle Pain • Cytokines: the Future
Nociceptive vs. Neuropathic Pain Neuropathic Pain2,3 Nociceptive Pain (Inflammatory?)1 Other “Mixed” Pain Types? CRPSII* Postherpeticneuralgia (PHN) Postoperativepain Trigeminalneuralgia Arthritis Neuropathic low back pain Sickle cellcrisis Mechanicallow back pain Central post-stroke pain Distalpolyneuropathy (e.g., diabetic, HIV) Sports/exerciseinjuries *Complex regional pain syndrome type II. 1. Portenoy RK, Kanner RM. In: Pain Management: Theory and Practice. Philadelphia, PA: FA Davis Company; 1996:4.2. Merskey H, Bogduk N, eds. Classification of Chronic Pain. 2nd ed. Seattle, WA: IASP Press; 1994. 3. Galer BS, Dworkin RH. A Clinical Guide to Neuropathic Pain. Minneapolis, MN: McGraw-Hill; 2000.
The BIOMEDICAL Model • Pain as a sensory event reflecting underlying disease or tissue damage
Gate Control Theory Melzack R. In: Cousins MJ, Bridenbaugh PO, eds. Neural Blockade in Clinical Anesthesia and Management of Pain. 3rd ed. Philadelphia, Penn: Lippincott Williams & Wilkins; 1998.
Gate Control Theory Sensory Affective Evaluative Melzack R, Wall PD. Science. 1965;150:971-976.
Enteroceptive Sensations • Pain • Thirst • Hunger • Thermoception • Neurophysiologic changes • Neurochemical changes
Biological Functions of Pain Sherrington (1906) Exteroceptive: Interoceptive: Escape and avoidance of external threats protection of injured or dysfunctional tissues that disrupt homeostasis Price DD et al. Pain 2003, 106.
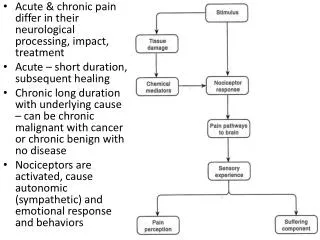
Physiological Pain • Initiated and by specialized sensory nociceptors innervating peripheral tissues and responding only to noxious stimuli • Projects to spinal cord and cortex • Activates reflex withdrawal, increase in arousal, emotional, autonomic and neurohumoral responses
Healing With Plasticity Normal Healing Allodynia Pain Relief Hyperalgesia Chronic Pain The Role of Plasticity in Chronic Pain Injury Acute Pain Adapted from Marcus DM. Am Fam Physician. 2000;61:1331-1338.
Neuronal Plasticity and Pain • Normal adaptive function • Neurons detecting and transmitting pain display “plasticity” • A capacity to change function, chemical profile, or structure • A response to painful stimuli and inflammation • A contributor to altered sensitivity to pain • When persistent can lead to permanent neuropathic pain Woolf CJ, et al. Science. 2000;288:1765-1768.
Pain Pathophysiology • Nociceptive pain • Believed to be related to ongoing activation of an intact nervous system by tissue injury • Somatic • Visceral • Neuropathic pain • Believed to be related to aberrant somatosensory processing in the peripheral nervous system, the central nervous system, or both
Nociception • Transduction: detection of noxious or damaging stimuli • Conduction: passage of resulting sensory input from peripheral terminals to the spinal cord • Transmission: synaptic transfer of input to neurones within specific laminae of DH
Physiology of Pain Perception1-3 Brain Perception DescendingPathway AscendingPathway SpinalCord C-Fiber α-β Fiber DorsalHorn α-δ Fiber Transmission/Modulation Conduction DorsalRootGanglion PeripheralNerve Transduction Injury 1. Galer BS, Dworkin RH. A Clinical Guide to Neuropathic Pain. Minneapolis, MN: McGraw-Hill; 2000. 2. Irving GA, Wallace MS. Pain Management for the Practicing Physician. New York, NY: Churchill Livingstone; 1997.3. Woolf CJ, et al. Ann Intern Med. 2004;140:441-451.
Classification of Fibers in Peripheral Nerves Lloyd /Hunt Diameter (µm) Letter System Conduction velocity (m/sec) Myelin Receptor/ ending 12-20 - 70-120 + Muscle spindle primary endings I-a 12-20 - 70-120 + Golgi Tendon organs I-b - 12-20 A-α 70-120 + Muscle efferents (extrafusal) II 6-12+ A-β 30-70 + Encapsulated endings;Merkel - 2-10 A-γ 10-50 + Muscle efferents (intrafusal) III 1-6 A-δ 5-30 + A-δ specific & polymodal; cold; hair; visceral (+/-) - <3 B 3-15 + Preganglionic autonomic IV <1.5 C 0.5-2.0 No C-nociceptors; C-polymodal; warmth, mechano;postganglioic autonomic; enteric nerve fibers Adapted from Nolte J. The human bran. St.Louis: Mosby, 1999:213.
Conduction Velocity: Aδ & C fibers • Aδ (Fast pain)1 • C-fibers (Slow pain)1 • Age related impairment in fast pain fibers2 • Julius D, Basbaum A, Nature 2001(413). • Chakour M,, et al. Pain 1996; 64:143.
Receptors Non-painful stimuli: • Specificity for a particular stimulus • High degree of gain to amplify weak signals • Rapid adaptation to increasing intensities Painful stimuli: • Specificity less important • High threshold receptors: thermal, chemical and mechanical stimuli (polymodal) • Threshold for firing may decrease Kidd, Urban. Br J of Anaesth 87, 2001.
C-fiber Small diameter Slow conducting Unmyelinated 1. Proinflammitory peptides Subst P CGRP Lamina I/II * tissue inflammation (NGF) 2. Specific enzymes/ Lectin IB4 *chronic neuropathic pain (GDNF) A-δ Medium diameter Fast conducting Lightly myelinated Polymodal Type I Long response latency > 50°C Persistent pain 2. Type II Short response 43°C Initial burn Cutaneous Caterina, Cur Op in Neurobiology (9), 1999.
Primary Afferent C & Aβ Fibers Sensation Mediated Fibre Class Threshold For Activation Principal Transmitters Receptors Engaged Physiological Pathological C High SP/NKA CGRP EAA NK CGRP NMDA AMPA mGlu Noxious (pain) Highly noxious (hyperalgesia) Cold Allodynia (pain) Aβ Low EAA AMPA Innocuous (no pain) Mechanical allodynia Millan, Progress in Neurobiology, 1999.
Receptor types on sensory neurons Transduction mechanism Example Cellular effect Ligand-gated channel Capsaicin-heat Excitation H , 5HT, ATP Glutamate, GABA-A G-protein linked GABA-B Inhibition of Opiated, Adenosine transmitter & Adrenoreceptors peptide release NPY, 5HT Bradykinin(B2) Excitation Histamine (H1) and/or Adrenoreceptors (α2) sensitization PGE2 Tyrosine kinase linked NGF (Trk A) Control of gene expression Bevan S. Textbook of Pain, 4th ed. Wall, Malzack, 1999.
Ion Channels • Dynamic, constantly changing • Plasticity reflects sensitivity needed for survival • Injury: amygdala, hippocampus, and DRG • Normal peripheral nerves (resist) • Demyelination: density
Capsaicin/ Vanilloid Purinergic (P2X) Receptors
Receptors Vanilloid (VR-1) Acid-sensing (ASIC) Purinergic (P2X) Cannabinoid Ion Channels Sodium TTX-S TTX-R Calcium Ion Channel Linked Receptors Kidd BL, Urban LA, Br J of Anaesthesia (1). 2001.
Nociception in Other Organs • Less differentiation • Autonomic component • Poorly localized • Referred pain • Absence of Aβ in viscera • Skeletal muscle: group III, group IV • Joint: group III & group IV respond to stretch
Psychophysics Not evoked from all viscera Not always linked to injury Referred to body wall Diffuse & poorly localized Intense motor & autonomic reactions Neurobiology Not all innervated by “sensory receptors” Functional properties of afferents Viscerosomatic convergence in CNS Few “sensory” visceral afferents, diverge CNS Warning system, capacity for amplification Visceral Pain Cervero F, Laird J, Lancet 353, 1999.
Siddal, Cousins. Neural Blockade in Clinical Anesthesia and Management of Pain, Third Ed.,1998.
Inflammation • Redness (rubor) • Heat (calor) • Swelling (tumor) • Loss of function (function lasea) • Pain (dolor)
Inflammation • Macrophages: • Cytokines(IL1, IL6, TNF-α) • Nerve Growth Factor • Damaged Cells: • ATP and protons • Mast Cells: • Histamine, serotonin, prostaglandins, arachidonic acid metabolites • Upregulation of receptors • VR1, SNS, SNS-2 & Peptides • Phenotypic Switch ( A-fiber into C-fiber) Jensen et al. Acat Anaesthesiol Scand 45, 2001.
Inflammation • Short-term • Modifications in excitation & sensitization of peripheral sensory terminals • Longer-term • Changes in properties of afferents • Decrease in threshold for firing • Increase in excitability of spinal neurons Mamet et al. J of Neuroscience, 22(24), 2002.
Hyperalgesia Sensitization pain threshold threshold for response pain to suprathreshold response to stimuli suprathreshold stimuli Spontaneous pain Spontaneous activity
SENSITIZING ‘SOUP’ Hydrogen Ions Histamine Purines Noradrenaline Potassium Cytokines Bradykinin Prostaglandins NGF Leukotrienes 5-HT Neuropeptides Peripheral Sensitization Tissue Damage Inflammation Sympathetic Terminals Woolf, Chong. Anesth. Analgesia (77), 1993.
Histamine Peripheral Sensitization SKIN Plasma Extravasation Vasodilation TNF-α IL-6 LIF Macrophage Mast Cell TissueDamage Pressure ? Bradykinin Heat 5-HT3 H+ PGE2 ATP NGF IL1ß 5-HT3 H1 EP B1/B2 IL1-R TrkA P2X ASIC VR1 H+ Ca2+ Peripheral Nerve Terminal (PKC) PKA PKC TTXs Gene Regulation TTXr (SNS/SNS2) TTXr Sub P Adapted from Woolf CJ, et al. Science. 2000;288:1765-1768.
With permission. Jensen TS et al. Acta Anaesth Scand, 45, 2001.
Mechanisms of Nociceptive Central Pain • Autosensitization of receptors • Ectopic firing of DRG cells • Calcium-induced molecular cascades from excess glutamate • Phenotypic change of A-β cells and DRG • Changes in gene expression of sodium channels and neuropeptides • Anatomic changes at dorsal horn Schwarzman et al. Neurological Review, 58, 2001.
Mechanisms of nociceptive central pain • Autosensitization of receptors • Ectopic firing of DRG cells • Calcium-induced molecular cascades from excess glutamate • Phenotypic change of A-β cells and DRG • Changes in gene expression of sodium channels and neuropeptides • Anatomic changes at dorsal horn Schwarzman et al. Neurological Review, 58, 2001.
Neuropathic Pain Is Defined as… …Pain caused by a lesion or dysfunction of the nervous system1 Nerve sensitization or damage can be located in the peripheral or central nervous system1 Manifests with sensory symptoms and signs2 May have both positive and negative sensory and motor symptoms and signs2 1. Merskey H, Bogduk N, eds. Classification of Chronic Pain. 2nd ed. Seattle, WA: IASP Press; 1994.2. Backonja MM. Anesth Analg. 2003;97:785-790.
Examples of Peripheral vs. Central Sensitization Central sensitization occurs as a result of increased nociceptor drive or disinhibition after nerve injury, leading to exaggerated dorsal horn response Inhibitory Input Is Downregulated To Brain Innocuous or Noxious Stimulus Innocuous Stimulus Dorsal Horn Neuron Dorsal Horn Neuron Increased Nociceptor Drive Disinhibition Sensory function after nerve injury with spontaneous firing along axon To Brain No Stimulus Pain Sensation Nociceptor Dorsal Horn Neuron Adapted from Woolf CJ, Mannion RJ. Lancet. 1999;353:1959-1964.
Persistent Pain as a Disease Entity: • Increase peripheral input: increase DH firing • Increase firing: increased NMDA, Ca, PKC, Nitric Oxide • Increase PKC, Ca: genetic changes • Increase NO: decreased GABA neurons • Increase Neurotrophins: sprouting Cousins, MJ, 2009 AAPM
Thermosensation Julius D, Proc 10th Word Conference of Pain, 2003.
Thermosensation TRP channel family • TRV2 >53 C Noxious heat • TRPV1 (Vanilloid) >43 C Heat, capsaicin, acid • TRPV3/TRPV4 >30-40 C Warm • TRPM8 (CMRI) >25 C Cold, menthol • TRPA1 <17 C Noxious cold Szalassi et al. Nature Rev 2007;6.
Cold 10-15% C & A-delta Specificity vs. modulation of excitatory & inhibitory channels K, Na, Ca channels CMRI (cold- and menthol-sensitive receptor) cloned TRP (transient receptor potential) Heat Capsaicin Vanilloid receptor subtype 1 (VR1 or TRPV1) Thermal activation threshold ~43°C Polymodal, influenced by a variety of substances Thermosensation Julius D, Proc 10th Word Conference of Pain, 2003.