Download
1 / 22
230 likes | 949 Vues
All Patient Refined Diagnosis Related Groups (APR DRG). AAHAM Presentation April 13, 2011 Presenter: Ronni Burkhart. Overview. Background Impact to Providers Implementation/Claim Adjustments Denied Claim Adjustments Communications Questions & Answers Contacts. APR DRG Background.

E N D
All Patient Refined Diagnosis Related Groups (APR DRG) AAHAM Presentation April 13, 2011 Presenter: Ronni Burkhart
Overview • Background • Impact to Providers • Implementation/Claim Adjustments • Denied Claim Adjustments • Communications • Questions & Answers • Contacts
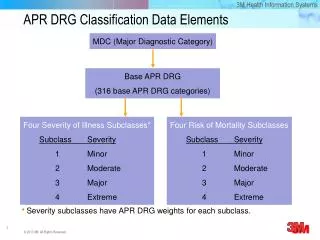
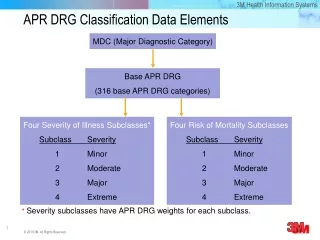
APR DRG Background • Classification system • reason for admission (procedure and diagnosis) • severity of illness (SOI) • Scaled payments
Impact to Providers • APR DRG rate letters – mid March • 7/1/2010 and after - APR DRG Version 27 • Prior to 7/1/2010 - Grouper 23 • Day outliers • High cost outlier can apply to any DRG • Up to 25 procedure and 25 diagnosis codes can be used • Birth weight - Value Code 54 or via diagnosis codes 764 through 779 • Otherwise assumed normal
Impact to Providers • New Error Status Codes (ESCs) 0582 VC 54 PRESENT/NO BIRTH WEIGHT ON CLAIM 0583 VC 54/BIRTH WEIGHT IS NOT NUMERIC 0584 VC 54/BIRTH WEIGHT MUST BE WHOLE NUMBER 0586 BIRTH WEIGHT IS GREATER THAN 4-DIGITS 0587 BIRTH WT. < 200 GRAMS OR > 7000 GRAMS 0982 ADMIT DATE IS PRIOR TO THE BABY'S DATE OF BIRTH 2125 RECIPIENT HAS PH MA MCO COVERAGE ON ADMIT DATE 4286 APR DRG 956 - UNGROUPABLE 4287 APR DRG 955 - UNGROUPABLE 4288 PROV BASE APR DRG RATE MISSING OR FOUND VALUE ZERO 4292 HIGH COST OUTLIER PRICING 4293 APR DRG 956 - DIAG CANNOT BE USED AS PRIMARY 4294 APR DRG 956 - RECORD DOES NOT MEET ANY DRG CRITERI 4295 APR DRG 956 - INVALID DISCHARGE STATUS 4296 APR DRG 956 - INVALID PRIMARY DIAGNOSIS 4297 APR DRG 956 - NEWBORN AGE/BIRTH WT CONFLICT 4299 MDC 14 WITH NON-MATERNITY APR DRGS
Implementation/Adjustments • Implemented March 4, 2011 • 7/1/2010 – 10/31/2010 - RA dated 3/21/2011 • 11/1/2010 – 3/3/2011 - RA dated 3/28/2011 • Wildcard – RA dated 4/11/2011 • ICN beginning in “52”
Denied Claim Adjustments • Some “52” adjustments will deny because the diagnosis code was unique to Grouper 23 and is no longer valid 4040 PRIMARY DIAGNOSIS CODE NOT ON FILE FOR DOS 4041 SECONDARY DIAGNOSIS CODE NOT ON FILE 4042 THIRD DIAGNOSIS CODE NOT ON FILE 4043 FOURTH DIAGNOSIS CODE NOT ON FILE 4044 PROC CODE NOT COMPENSABLE FOR PROV TYPE/SPEC 4045 PROV TYPE/SPEC/PROC CODE/MODIFIER INVALID 4046 PT/SPECIALTY/PLACE OF SERVICE COMBO IS INVALID 4047 FIFTH DIAGNOSIS CODE NOT ON FILE 4048 SIXTH DIAGNOSIS CODE NOT ON FILE 4049 SEVENTH DIAGNOSIS CODE NOT ON FILE 4050 EIGHTH DIAGNOSIS CODE NOT ON FILE 4051 DIAGNOSIS CODE NOT ON FILE • Providers MUST correct the diagnosis codes on the original claim based on 2010 diagnosis codes and resubmit to be in compliance
Denied Claim Adjustments • Some “52” adjustments will deny because the procedure code was unique to Grouper 23 and is no longer valid 4053 PRINCIPAL ICD-9 PROCEDURE CODE NOT ON FILE OR NOT 4054 2ND ICD-9 PROCEDURE CODE NOT ACTIVE ON DOS 4055 THIRD PROCEDURE CODE NOT ACTIVE FOR DOS 4056 FOURTH PROCEDURE CODE NOT ACTIVE FOR DOS 4057 FIFTH PROCEDURE CODE NOT ACTIVE FOR DOS 4058 SIXTH PROCEDURE CODE NOT ACTIVE FOR DOS 4067 NON-COVERED ICD-9 PROCEDURE CODE • Providers MUST correct the procedure codes on the original claim based on 2010 procedure codes and resubmit to be in compliance
Communications • Provider Quick Tip #102 http://www.dpw.state.pa.us/ucmprd/groups/webcontent/documents/communication/p_003129.pdf • Full Provider Teleconference http://www.dpw.state.pa.us/ucmprd/groups/webcontent/documents/presentation/p_004128.pdf • PA Bulletin http://www.pabulletin.com/secure/data/vol40/40-26/1177.html • FAQs – 02.04.2011 http://www.dpw.state.pa.us/ucmprd/groups/webcontent/documents/document/p_004120.pdf
Communications • Inpatient Hospital Provider Handbook and Billing Guide http://www.dpw.state.pa.us/publications/forproviders/promiseproviderhandbooksandbillingguides/index.htm • Appendix I – APR DRG Pricing http://www.dpw.state.pa.us/ucmprdc/groups/webcontent/documents/document/p_010882.pdf • APR DRG Relative Weights http://www.dpw.state.pa.us/ucmprd/groups/webcontent/documents/document/p_004089.pdf
Questions & Answers Is there any plan for the MA HMO plans to also move to APR-DRGs? At this time, there is no requirement or deadline for the MCOs to implement APR-DRGs. Do the adjustments need to be re-filed within 365 days from the date of service? Yes, if the department initiated claim adjustment denied, you will need to correct the original claim within 365 of the end date of service.
Questions & Answers Can providers choose to take “no action” on the adjustments when they error? (For example, keeping original payment) No, if the department initiated claim adjustment denied, you will need to correct the original claim within 365 of the end date of service. When do we have to re-code and resubmit the claims? Department initiated mass adjustments related to APR DRG that denied should be tracked back to the original claim and the original claim should be corrected and resubmitted as soon as possible.
Questions & Answers When the claims are reprocessed by MA and some may deny due to incompatible diagnosis coding, if we do nothing, will MA leave the original payment in place or will they retract the original payment expecting that we will resubmit the claim? The department is finalizing the grace period that will be afforded to providers. It is in the providers’ best interests to correct the denied adjustments as soon as possible. When will Promise be able to accept the 4 digit DRG code that contains the severity of illness as the last digit? According to the MA Companion Guide the DRG number is not required on a claim; however, our systems are populating the SOI which is causing the claim to reject. At this time, the Department does not have any plans to support the inclusion of SOI on submitted claims.
Questions & Answers Most of the accounts are paying us an additional amount but we have had some that are paying less. And we are not questioning them. But we have also encountered some secondary to Medicare claims in which the original claim did not approve to pay the Medicare deductible, however on the reprocessing they are now paying the Medicare deductible, and then some that did pay the deductible and now on the reprocessing they are not paying the deductible. I just want to make sure whether or not we should be questioning these. Using the upcoming question related to Medicare pricing, you will see that when the Medicare paid amount exceeds the MA allowed amount, no payment is made to the provider. As the MA Allowed amount increases, such as many of the cases under APR DRG, and exceeds the Medicare paid amount, it is more likely that the difference between MA Allowed and Medicare paid amount will be paid up to the amount of Medicare deductible and Medicare coinsurance.
Questions & Answers Can you explain the outlier formula? Step 1 – Calculate Base = Hospital Rate x APR DRG/Severity Weight $4,779.19 x 8.61363 = $41,166.1743597 Step 2 – Calculate Hospital Cost = Hospital Cost to Charge Ratio x Billed Amount 0.5158 x $175,550.91 = $90,549.159378 Step 3 – Calculate Potential Outlier = Hospital’s Cost – Base APR DRG $90,549.159378 - $41,166.1743597 = $49,382.9850183 Step 4 – Calculate Possible High Cost Outlier = Potential Outlier – Cost Outlier Threshold If >0, go to step 5 $49,382.9850183 - $24,000.00 = $25,382.9850183 If <0, no high cost outlier Step 5 – Final Outlier = Possible High Cost Outlier x APR DRG/Severity Outlier Percentage $25,382.9850183 x .80 = $20,306.38801464 Step 6 – MA Allowed Amount = Base + Final Outlier $41,166.1743597 + $20,306.38801464 = $61,472.56237434 or $61,472.56 Exceptions: Two Day Per Diem Pricing Transfer Pricing Interim Pricing
Questions & Answers Can you review how MA calculates the allowable secondary to Medicare? Step 1 – Calculate Medicare Paid = Medicare Approved – Medicare Deductible – Medicare Blood Deductible – Medicare Coinsurance $7,574.59 - $1,100.00 - $0.00 - $0.00 = $6,474.59 Step 2 – Calculate MA Allowed (see previous question) $12,111.99 Step 3 – Compare: MA Allowed – Medicare Paid $12,111.99 - $7,574.59 = $4,537.40 And Medicare deductible + Medicare Coinsurance $1,100.00 + $0.00 = $1,100.00 Step 4 – Pay the lesser of step 3 $1,100.00
Questions & Answers What field on the UB/837 will identify an emergent admission? (question related to non-contracted MCO's that follow MA guidelines.) Providers should use the Admission Type field. Enter 1 for an emergency admission Enter 2 for an urgent admission Enter 3 for an elective admission Enter 4 for a newborn admission Enter 5 for a trauma admission. (The Department recognizes Trauma Admission, Admission Type Code 5 as an emergency admission)
Questions & Answers I was expecting a payment related to hospital assessment funding from the Department of Public Welfare and did not receive one. Why? One potential payment made by the department was related to the reprocessing of fee for service inpatient claims with dates of discharge 7/1/2010 and later under the new APR-DRG logic. Based on claim specific details, you may have seen a payout related to this portion of the initiative beginning with your March 21, 2011 remittance advice. If you did not receive a payment related to this portion of the department’s initiative and only provide inpatient services to Medicaid recipients through an agreement with a contracted Managed Care Organization (MCO), please contact the MCO to determine if and when you may receive an APR-DRG related payment. In addition, you may receive one or more of the following payments related to the hospital assessment funding based on the tentative schedule on the next slide.
Contacts PROMISeTM Website http://promise.dpw.state.pa.us DPW Website http://www.dpw.state.pa.us Provider Service Center (Billing Questions) 800.537.8862 Provider Assistance Center (Technical Support) 800.248.2152